The Basics of Hypertrophic Cardiomyopathy
Hypertrophic Cardiomyopathy (HCM) is the most common genetic heart disease in the United States, with 1 in 500 (0.2%) diagnosed with the condition worldwide. Learn about the basics: signs, symptoms, and diagnosis of HCM with guest Jane A. Linderbaum MS, ARNP, FACC, Associate Professor of Medicine at the Mayo Clinic. We have a guest host for this episode, Dr. Eileen M. Handberg, PhD, ANP-BC, FACC, PCNA President.
Thank you to Bristol-Myers Squibb for supporting this podcast episode.
Episode Resources
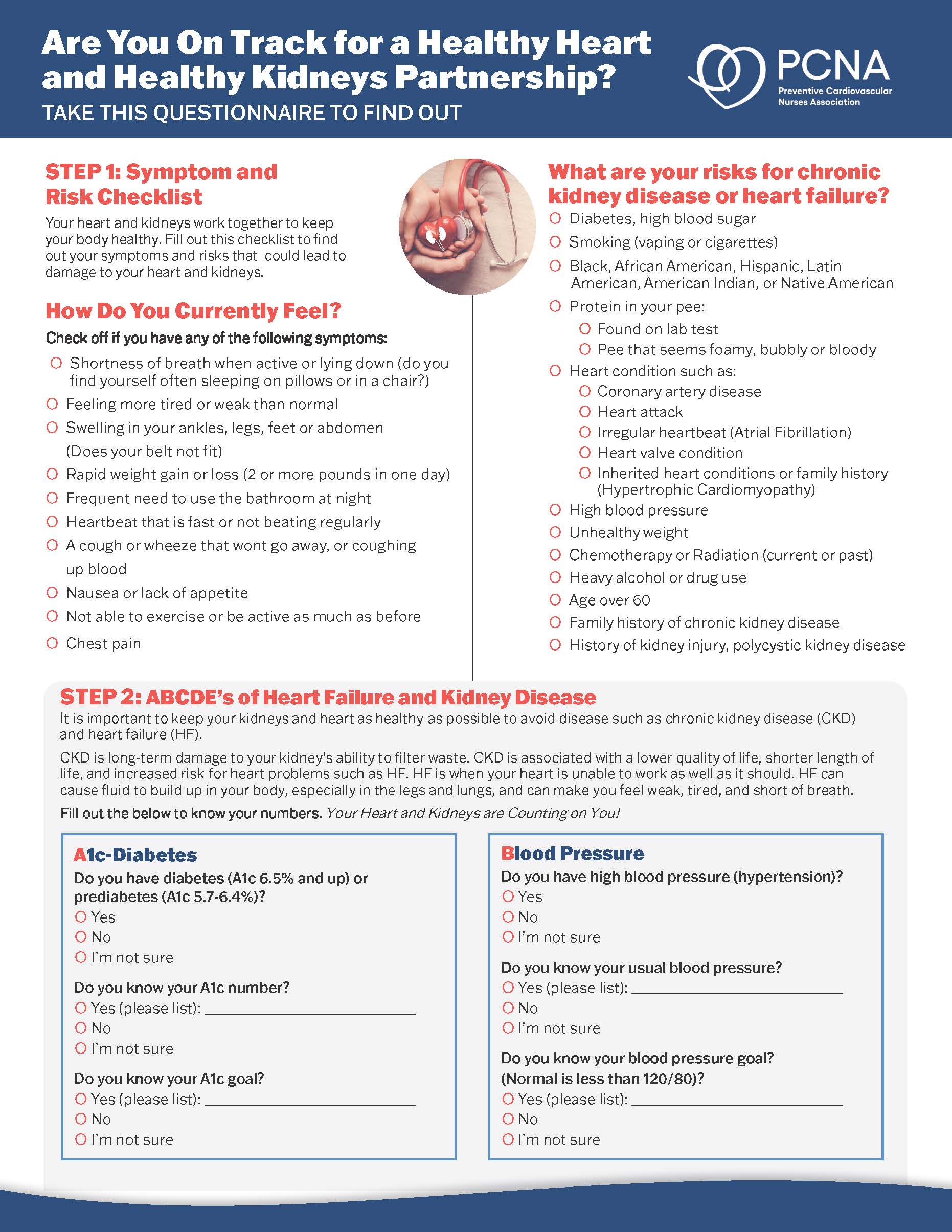
- Patient Education Resource: Hypertrophic Cardiomyopathy: What You Need to Know
Welcome to Heart to Heart Nurses, brought to you by the Preventive Cardiovascular Nurses Association. PCNA’s mission is to promote nurses as leaders in cardiovascular disease prevention and management.
Dr. Eileen Handberg (00:18):
Welcome to PCNA’s Heart to Heart Nurses podcast. I’m your host, Dr. Eileen Handberg. I am currently the president of PCNA and a nurse practitioner at the University of Florida in Gainesville and director of the cardiovascular clinical trials program.
I’m excited today to be here as part of this podcast series. This first podcast about hypertrophic cardiomyopathy is going to be mostly about symptom recognition and diagnosis.
Hypertrophic cardiomyopathy, or HCM, is the most common genetic heart disease in the United States, with one in 500 or 0.2% diagnosed with a condition worldwide.
In HCM the wall of the heart’s left ventricle is thicker than normal, reducing the heart’s ability to pump blood efficiently, and in severe cases can obstruct blood flow to the rest of the body.
HCM affects men and women equally, regardless of age. Diagnosis can be challenging as symptoms of HCM are variable, even within the same family. Some people who have HCM are asymptomatic and the disease does not affect their lives. Other individuals have severe symptoms and complications often during exertion.
Our guest today is Jane Linderbaum, Associate Professor of Medicine at Mayo Clinic in Rochester. She’s associate editor of AskMayoExpert and practices as a nurse practitioner in structural heart disease and valvular heart disease and cardiomyopathies.
For this episode, we’re going to be covering the basics of HCM. Jane, in the diagnosis of HCM, is there a typical patient in terms of how they present?
Jane Linderbaum (02:11):
Great question, Dr. Handberg, and thanks for the invitation to be with this audience today. So I think importantly, you gave a great introduction. And when you think about the fact that two people per 1000 people have hypertrophic cardiomyopathy and the majority of people with hypertrophic cardiomyopathy are asymptomatic. So now we’re down to a small number of patients who have symptoms. And again, most individuals with hypertrophic cardiomyopathy don’t even have symptoms. So sometimes it’s a little bit of a difficult diagnosis.
Patients that present with symptoms or have clues in their family that makes you be concerned that they may have hypertrophic cardiomyopathy sometimes will present with an abnormal ECG or a heart murmur. Symptoms that might be associated with hypertrophic cardiomyopathy might include exertional dyspnea, syncope, dizziness, lightheadedness, sometimes fainting in some individuals.
There are some individuals that actually have a syncopal event with injury at first presentation. Some individuals have chest pain similar to typical angina that we see in our practices. And some patients have palpitations. And as you might imagine, some patients have a myriad of those things presenting at different times throughout their presentation.
Dr. Eileen Handberg (03:33):
So when you have a patient… That’s every cardiology patient you just described.
Jane Linderbaum (03:37):
You bet.
Dr. Eileen Handberg (03:39):
So what is a normal ECG, and pretty standard these days to get an echocardiogram in most patients, especially if they have a murmur? But just generally, the lightheaded spells, is it heart failure I think would probably be a more common differential that we would be going down. So when you get the echo, is that then where you get the true signal that it may be HCM?
Jane Linderbaum (04:10):
Yeah, great question once again. So very often you’d see evidence of left ventricular hypertrophy on the 12 lead electrocardiogram, and then your echocardiogram very often would help confirm the diagnosis. And you’d see left ventricular and septal hypertrophy far higher than you would see with other diseases or conditions that might cause an increase in the size of the left ventricle.
Jane Linderbaum (04:34):
Again, we’re talking about thickness of the left ventricle and septum, and the ventricle itself would not be generally enlarged like you would see in heart failure. So for example, on a chest x-ray, which you may also get in the evaluation of any cardiac patient for that matter to rule out structural heart disease. On the chest x-ray, a patient with hypertrophic cardiomyopathy may have a normal size heart but a thickened left ventricle or thickened, abnormally thickened septum.
Dr. Eileen Handberg (05:05):
And so how often do you get patients who present with vague symptoms, and then when you’re doing the history, you find that family connection for odd things in family history that nobody associated with being cardiac? Our histories of our families 50, 75 years ago are very different than how we know about our medical histories now. We have much more testing and people understand a lot of conditions a lot better. And back in the day, my uncle died suddenly or somebody died in a car accident, with no thought that the cause of the car accident could have been a sudden cardiac death or something like that.
Do you get these patients who you say, “Gosh, it looks like you have HCM.” And then the history goes in that direction?
Jane Linderbaum (06:12):
Very much so, and certainly when a patient has a family member who died unexpectedly at an early age or really of an unknown cause or condition, that definitely perks my ears up and makes me think, Hmm.
And I would definitely talk to that patient more about family history and if they’ve any known or unknown cardiac conditions or earlier sudden cardiac death. And that would definitely make me think about the genetic disease of hypertrophic cardiomyopathy, and really looking at first relatives of the individual, of my individual patient or the proband as you might call, and really see if there’s a mother or a sibling who has known or perhaps expected hypertrophic cardiomyopathy.
Dr. Eileen Handberg (06:59):
So we talked a little bit about the ECG and the echo, what other tests… So you get an echo and there’s some hypertrophy of the septum and the LV, is that the definitive diagnosis? Are there other testing modalities that need to be undertaken to confirm the diagnosis or the extent, or how does that work?
Jane Linderbaum (07:23):
So yeah great, another fantastic question, of course. And certainly, if you are in a practice and you get a electrocardiogram and you have left ventricular hypertrophy on the electrocardiogram, and then the left ventricle and or the septum looks thickened on echo and your patient comes in with symptoms or a murmur, you’ve pretty much got the diagnosis of hypertrophic cardiomyopathy.
And in those patients, they definitely deserve a referral to a hypertrophic cardiomyopathy center to really help you put the whole package together and or the genetic screening and the discussion with the patient and family regarding activity, outlook, follow-up, medical therapy, and certainly any other advanced testing that would need to be made at that time.
Those are the patients that based on their symptoms, you may order additional tests. For example, if the patient gives you a history of any syncope, pre-syncope, fainting, palpitations, you definitely would want to get a Holter monitor on that individual. And probably at some point consider a cardiac MRI as well.
So when we think about goals of therapy for patients with hypertrophic cardiomyopathy once we have the diagnosis confirmed, it’s really management of symptoms. And so symptom management is the number one thing we want to do. And then the second most important thing is a prevention of sudden cardiac death.
So prevention of symptoms, prevention of sudden cardiac death, and identifying that patient’s individual risk factors for sudden cardiac death are very important and really paramount to the management of that patient.
Importantly, we’re still talking about a population where most patients are asymptomatic, but we’re definitely talking about a population of patients where it’s going to be very important for your patient and their family to understand their condition very well, and how both they and their family members should be screened moving forward.
Dr. Eileen Handberg (09:17):
So before we go on to the family, can you give us a definition? What defines obstructive versus nonobstructive?
Jane Linderbaum (09:29):
Another fantastic question. So most patients with hypertrophic cardiomyopathy are non-obstructive, and that just means that they don’t have an obstruction with the outflow. So for example, when the blood ejects from the left ventricle through the aortic valve, there’s a thickening of the septum prior to the aortic valve that causes an outflow murmur. So these would be a patient that has a murmur of obstruction, and sometimes that can decrease the blood flow or limit the blood flow out to the rest of the body, which definitely gives that patient pre-syncope and lightheadedness, dizziness, and sometimes activity limitation.
There are also patients that have an increased pressure and can cause some obstruction up to the left atrium, and they can get dyspneic with exertion as well. So an obstruction is when the blood is limited and notified by a murmur, or that’s your tip-off as a clinician that a patient has an obstruction. When they have an obstruction, the goal of therapy would be to see if we can medically manage that and decrease the degree of obstruction, such that we’re improving the symptoms for that patient.
So when we talk about doing that, the mainstay of medical therapy for patients with hypertrophic cardiomyopathy is beta-blockade. So the goal with beta-blockade is to decrease the outflow murmur, which would decrease the likelihood of symptoms associated with a dynamic outflow obstruction. And certainly beta-blockers, we all know that drug well, we use them in lots of other patients for other diseases and conditions also. But it changes or decreases the contractility and the heart rate response to exercise.
So in fact that lowers the degree of obstruction and many patients get better or have less symptoms when they’re on beta-blocker therapy for the treatment of their hypertrophic cardiomyopathy. Beta-blockers, they’re effective in about 70 to 80% of patients with hypertrophic cardiomyopathy. So we’re driving home the take-home message here that this is really a pretty manageable condition if we can get effective symptom relief in about 70 to 80% of our patients.
We might monitor the beta-blockers and titrate the beta-blockers up to tolerated doses with a goal resting heart rate about 60 beats per minute. We get that resting heart rate less than 60 beats per minute, then that patient with activity and or exercise is less likely to have symptoms.
When we talk about symptoms, we also can talk about dynamic outflow obstruction. So for example, when a patient is dehydrated or certainly exposed to hot or heated conditions, for example, think sauna, hot tub, whirlpool, their outflow obstruction actually may worsen. And so we’ll instruct our patients and educate our patients to avoid conditions that might increase their outflow obstruction and make them thus more symptomatic.
For patients unable to tolerate beta blockers we might also use calcium channel blockers such as Verapamil works really well. And sometimes we use those in combination. The goal is like when you think about heart failure titrating to maximally tolerated doses, we do the same thing with our patients with hypertrophic cardiomyopathy. So for example, Verapamil either for a patient who can’t tolerate a beta-blocker or in addition to a beta-blocker, Verapamil’s typically helpful in about 60% of patients.
Certainly, we want to make sure that they’re tolerated at doses that they can tolerate well. And again, it decreases the degree of obstruction and decreases overall contractility and heart rate response to exercise.
So reminding everybody, as we think about hypertrophic cardiomyopathy, you’ve got a big… A thickened heart muscle without the heart itself being enlarged. So the chambers or the filling chambers, the ventricles of the heart are much smaller. So there’s less blood that can fit into a hypertrophy ventricle because the cavity is smaller. The heart itself isn’t larger, like with a heart failure patient, it’s a different disease or condition.
These patients typically have a hyperdynamic LV, so it’s not uncommon at all that their injection fractions in the 70s, 80s sometimes. And so you can certainly slow their heart rate which might decrease their ejection fraction, give them more filling time and minimize the diastolic dysfunction of that ventricle. And then you have success with some symptom relief.
Dr. Eileen Handberg (14:07):
Wow, that’s fabulous. I’m so glad we have you on this podcast today. I’m learning a lot. We’ve been talking to Jane Linderbaum about hypertrophic cardiomyopathy. We’ll be back after a quick break.
Dr. Eileen Handberg (14:19):
We’re back to discuss more about hypertrophic cardiomyopathy with Jane. Jane, can we pick up with we’ve been through the presentation of HCM, how generic the symptoms may be, that you really have to do a good history and physical. We talked about the goal of therapy being symptom management.
You talked about using beta-blockers, calcium antagonists. What about the risk that we hear about a lot, which is the sudden cardiac death risk assessment and ICD? We always hear a lot about the dramatic cases, those are the ones that make the press, make YouTube and all of that kind of stuff.
How often does that really happen, it’s a small percentage of the population that had the disease anyway. We see a lot of this with athletes, and maybe talk a little bit about that.
Jane Linderbaum (15:23):
Yeah, great. As I’m thinking about that, we talked about our goals of therapy are symptom management and prevention of sudden cardiac death. We talked about symptom management with the addition of beta-blockade and calcium channel blockers, such as Verapamil. Other medications that can be used are Disopyramide, and that can be used for symptomatic outflow, tract obstruction as well. A little bit tricky in elderly patients because it does have some anticholinergic effect, and typically is started in most hospitalized settings to make sure patients are on appropriate doses.
And then there’s a new class of drugs that really has some great potential advantages. The myosin inhibitors that we’ve all heard about and was recently presented with the VALOR-HCM trial, and that’s really shown to decrease obstruction for many patients and well-tolerated. And certainly when patients get to maximally tolerated doses of medications and that does not work, then we’re down to advanced therapies. And it looks very promising for our future.
We’re going to need more studies, but we have a new tool in the toolbox with the addition of the myosin inhibitors. And so we’re really looking forward to that.
In addition to medical therapy for patients with hypertrophic cardiomyopathy, at the initial onset, we do want to do a sudden cardiac death risk assessment. And this is really an individualized assessment of that patient’s risk of sudden cardiac death and whether or not they might benefit from a defibrillator. And you calculate the five-year sudden cardiac death using the sudden cardiac death risk calculator, that was authored and put together by the American Heart Association and can be accessed online.
And you’re really looking at that patient’s individual risks. So, for example, the degree of myocardial hypertrophy, whether that patient has any personal or family history of sudden cardiac death or sustained ventricular tachycardia, and certainly patients in their initial assessment very often do have a Holter monitor or an extended event monitor recorder to see if they have any palpitations or sustained ventricular tachycardia.
Whether or not patients have symptoms, you definitely want to assess whether or not they’re having sustained ventricular tachycardia. Because if in fact, they are, there would likely be an increased risk for sudden cardiac death event. We would definitely be looking at all those factors together to calculate their individual sudden cardiac death risk.
So, number one, look at prior cardiac arrest or documented sustained ventricular tachycardia. Number two would be massive septal hypertrophy or ventricular hypertrophy greater than three centimeters. So you’ll measure the degree of hypertrophy, your echo will give you a reading on that.
Third would be family history of unexplained sudden death or sudden death due to hypertrophic cardiomyopathy. The fourth thing would be if they’ve had unexplained syncope in the last six months. The fifth thing would be non-sustained VT on a Holter monitor or exercise testing.
Any evidence of an apical aneurysm typically puts patients at an increased risk, and you would know that typically from your echocardiogram. If the patient had an ejection fraction less than 50%, that patients at increased risks for arrhythmia and sudden cardiac death. And importantly, if that patient has extensive myocardial disarray or gadolinium enhancements reported on your cardiac MRI, that would be a cardiac MRI. And you’d always order that with and without gadolinium.
And if you have myocardial disarray that’ll show up as late gadolinium enhancements on your cardiac MRI. And typically we know we’re at increased risk if the degree of myocardial late gadolinium enhancement in MRI is greater than about 15%. So most advanced MRI readings will give you a percent of late gadolinium enhancement on your MRI report. So that would be a red flag condition that your patient might be at increased risk for sudden cardiac death.
Like anything, a shared decision-making process with your patient and family members, looking at their personalized risk, taking that in comparison with the guideline recommendations and their decision on whether to proceed with a ICD based on their individual risk is an important conversation to have.
Dr. Eileen Handberg (20:07):
So since this is a condition that’s often asymptomatic, do you have trouble getting patients to have an understanding that they have something that needs to be treated? When you were talking about all this, it likens a little bit to me to hypertension. It’s relatively silent, it has deadly effects, but if you don’t feel like you have it or you have a little shortness of breath occasionally, do you have trouble getting patients to understand what they have and the benefits or risks of treatment?
Is that a challenge or I guess I’m thinking of all these patients, some are going to come in because they have something, some are going to be incidental findings. So I’m trying to get my head around how you have these conversations with these patients.
Jane Linderbaum (21:12):
So I think it’s a challenge we’ll continue to deal with when any patient has important or a potentially life-changing condition that’s asymptomatic. Think of the early days of the severe mitral valve regurgitation that presented in the severe phase, or you’re trying to urge a patient to proceed with an open chest surgery and they’re asymptomatic. And your goal is to prevent long-term sequelae of a disease or condition gone untreated.
And certainly, in a patient with hypertrophic cardiomyopathy, sometimes we’re unable to predict. And some patients, their first presentation will be following a sudden cardiac event. And you definitely want to prevent that whenever possible.
You commented earlier in the discussion about athletes and sudden cardiac death, and certainly when we think about professional athletes, and we’ve all seen those videos and reports and testimonials that they had a condition they didn’t know about. And their first quote symptom was in fact a sudden cardiac death episode. There are patients who with treatment we’re able to improve things for them and decrease their risk.
So for example, we can maybe sometimes decrease the ventricular tachycardia by treating their arrhythmia and or making sure that we’re controlling their outflow obstruction, but there’s really not a treatment for gadolinium enhancements because that myocardial disarray puts them at increased risk for arrhythmias moving forward. So there’s things we can treat and things we can’t treat.
We can’t treat or change your gene pool. We can’t treat or change the fact that your mother passed away at a young age from hypertrophic cardiomyopathy unexpectedly, those things we cannot change. And so we have to look at it at an individual basis and really say based on your current age and your current symptoms, here’s your risk for sudden cardiac death.
And we really need to look at where we might need to have you best protected. I do think that referral to a center of excellence is really important at least early on in some of these patients because you really want to have that discussion before a decision is imminent. So if I’ve met the individual and their family and have a relationship with them, and I’ve surveilled them over the years and now for example we see a progression of their disease or condition, it’s a much easier discussion when we need to move on to advanced therapies, that being an ICD and or sepal reduction therapy.
So, I think that’s important and another reason to look at a center of excellence early in the discussion with these patients because it’s a big decision if you are posed with it and need to make that decision.
But again, we do have good data on patients that benefit from ICD placement and patients who are typically going to do well. And certainly, the age of the individual and the progression of the disease helps us look at them and re-stratify them.
Dr. Eileen Handberg (24:06):
So we have two more podcasts coming in this area. The second is going to deal a little bit about the center, a lot about the centers of excellence. So we’ll get into that. And the last podcast is going to talk a lot about shared decision-making, and I think that’s extremely important and deal a little bit… Can we end up the discussion and talk a little bit about the genetics of this, and how do you approach patients to try and figure out, is there a genetic component, and where are we with gene testing for this disorder?
Jane Linderbaum (24:48):
That’s great. Thank you for that good question. We’re lucky because it’s now, fortunately, more readily available at a much lower cost, certainly centers of excellence in areas that have genetic counselors have been a huge asset to our practice and are able to keep up on this information and certainly evolving technology.
There’s about six or seven different genetic variants that have been associated with hypertrophic cardiomyopathy. The MIH seven is largely about 60% of genetic cardiomyopathies are associated with that gene type. There are also a variance of unknown significance that may or may not be related to hypertrophic cardiomyopathy, but we continue to learn more and more about that.
I think I can simplify genetic testing, and this is some of the discussions I have with patients. So again, if I’m the proband, if I’m the mother of younger children that is presenting with hypertrophic cardiomyopathy, I’d be the proband.
And if I were to have genetic testing, it’s not going to really change anything for me because I already know and I carry the diagnosis of hypertrophic cardiomyopathy, but it may very well be an asset in screening of my first-degree family members to identify whether or not a genetic cause can be attributed to my type of hypertrophic cardiomyopathy.
So for example, if I undergo genetic testing and they are able to identify a mutation, then I have a genetic cardiomyopathy. If my children and siblings were then tested, they either would have or not have the genetic variant associated with my cardiomyopathy. If they have the genetic variation then they are at risk for hypertrophic cardiomyopathy, and they would be at risk and they would need to have screening echoes on an annual basis to see if that condition or disease develops with them.
If mutation is not found in my children or siblings, that’s the end of it, no further testing would be needed for those individuals because they do not have the genetic variant and they would not be likely to develop hypertrophic cardiomyopathy.
Where I really find that is helpful, if I have nine children and four siblings, and I can identify that I have a genetic variant and I can identify that none of them do, that’s a lot of concern and a lot of echocardiograms that we probably don’t need to pursue.
However, if I have hypertrophic cardiomyopathy, I have genetic testing and they don’t associate it with a variant. We still need to do echo screening of my nine children and my siblings. And again, you know well that I don’t have nine children. This is a case study example. But definitely, I would need to continue the echo screening of my children, siblings, and any relatives or competing athletes to be sure. If hypertrophic cardiomyopathy is identified in any of them, they’re certainly at risk and would need an annual echo. If it’s not identified, we still don’t know if there’s a genetic variant, we just haven’t been able to identify. So it doesn’t eliminate that there’s one but we just haven’t been able to identify, so they would need to continue to be screened.
So, the genetic testing really what it does is it I think informs us to better treat our first-degree relatives and certainly has been, I think, helpful in pre-pregnancy counseling so that people know.
For example, if I had hypertrophic cardiomyopathy myself and my first-degree relative had carried that variant, there’s about a 50% chance that that would be passed on. And really important in pre-pregnancy counseling for individuals with hypertrophic cardiomyopathy and in families with hypertrophic cardiomyopathy.
Dr. Eileen Handberg (28:34):
Well, this session has been absolutely fabulous. I would like to thank Jane Linderbaum for sharing all her wealth of knowledge about HCM with our audience and look forward to our next two podcasts.
PCNA thanks Bristol Myers Squibb for their support of this non-CE podcast. PCNA is proud to offer educational opportunities like these to further our commitment to educate our members in an objective way, regardless of funding support.
(29:06):
Thank you for listening to Heart to Heart Nurses. We invite you to visit pcna.net for clinical resources, continuing education, and much more.
Topics
- Heart Failure
Published on
June 21, 2022
Listen on:

MS, ARNP, CNP, FACC, FPCNA
Related Resources