")
Treating inflammation in cardiovascular disease includes helping patients to understand the safety and efficacy of prescription and over-the-counter products. Joseph Saseen, Pharm D, FNLA, CLS discusses best practices in clinical decision-making, mechanisms of action, and guideline-based evidence for various anti-inflammatory medications.
Episode Resources
Welcome to Heart to Heart Nurses, brought to you by the Preventive Cardiovascular Nurses Association. PCNA’s mission is to promote nurses as leaders in cardiovascular disease prevention and management.
Geralyn Warfield (host): I’d like to welcome back our audience members today. We’re going to be speaking with Joseph Saseen, and Joseph, I’m going to go ahead and let you introduce yourself to our audience.
Joe Saseen (guest): Great. Thank you very much. My name is Joe Saseen. I’m a Professor and Associate Dean for Clinical Affairs at the University of Colorado. I’m a clinical pharmacist that works in a primary care clinic and focuses on cardiovascular risk reduction, so management of hypercholesterolemia, hypertension, and of course diabetes and a few other things that come in primary care.
I’m also active in the National Lipid Association and currently serve as the immediate Past President.
Geralyn Warfield (host): Well, obviously we could probably spend weeks speaking to you about your expertise in all kinds of topics related to things that our audience members are interested in, but I’m wondering if today we could [00:01:00] focus in on some common medications that are used to treat inflammation in cardiovascular disease.
Joe Saseen (guest): That’s a great question. And there’s a lot of treatments that people use to combat inflammation. And those include the typical list of things that we know to be anti-inflammatory drugs like NSAIDs, aspirin, colchicine, can be prescribed, and then some other emerging therapies.
The other end of that is there’s a lot of therapies that people use that are supplements that patients self-treat to combat inflammation. Even though these are commonly or perhaps, common medicines that might be used for inflammation, it doesn’t mean that they’re all proven to reduce risk of cardiovascular events or are even recommended to reduce cardiovascular events.
I think perhaps the biggest area though are our patients who are using over-the-counter supplements. I don’t consider those drugs because they’re not regulated by the FDA. But a lot [00:02:00] of them are being advertised and, I guess, marketed as anti-inflammatory treatments. And we have to be very careful with that because we’re dealing with an area that really is mostly unproven and, in some contexts, might be harmful.
Geralyn Warfield (host): So how might you, in clinical practice, address those misconceptions about the safety and efficacy of over-the-counter medications or over-the-counter supplements with our patients?
Joe Saseen (guest): I think it’s always best to be honest and tell patients what you know and what is the truth. The harder part is translating it into messages that they can understand.
With over-the-counter drugs, I view them very differently than over-the-counter supplements. Over-the-counter drugs are things like aspirin, or NSAIDs, or proton pump inhibitors–those kind of treatments. They are viewed as ‘medicines’ or ‘pure drugs’ according to the FDA. So, they go through safety and efficacy studies to prove that they are legitimate drug therapies. They [00:03:00] treat a medical condition. If they’re over-the-counter, it just means that they are able to be self-identified and self-administered by a patient who can identify the condition that it treats.
That’s very different than supplements.
Supplements are not drugs and they cannot be labeled to treat any condition. They can only have labeling that indicates they support a biologic function. And that is sort of a fine line and patients have a hard time sometimes understanding the differences that a pure drug treats a condition—some of them are over-the-counter, most of them are prescribed.
But supplements really are things that support a physiologic function, and have a high degree of variability in both what we know they do is long-term (meaning whether they work or not; we don’t always know); and we don’t always know whether a capsule that has the supplement, or the tablet that has the supplement, actually has anything in it unless it goes through own its own regulation. Because there is [00:04:00] no required oversight for supplements with regards to purity or ingredients. It’s all voluntary. The only thing that’s regulated is labeling.
Geralyn Warfield (host): So, do you find that because patients can purchase these, both over-the-counter medications and supplements on their own without a prescription, that that really contributes a lot to their misconceptions about the safety of them and their ability to do what they’re marketed?
Joe Saseen (guest): Absolutely. I think that if aspirin was a new drug right now, the FDA would not put it over-the-counter because of the known bleeding risk that we have with aspirin and the misuse of it, perhaps, in the wrong population.
But I think there is that implied faith that if something is over-the-counter, it’s safe. And that if something is a supplement or an herbal, that it’s mega-safe when actually it might not be. There are actually proven drug interactions with certain supplements. There’s proven side effects that are associated with supplements.
And [00:05:00] there’s also sometimes purity issues. I won’t say contaminants. I’m not overly concerned though I can’t rule it out that there’s contaminants and supplements, but purity could be. I could put whatever I want in a capsule and call it fish oil. It doesn’t even have to be from fish because it’s not going to be regulated.
Geralyn Warfield (host): So, we’re not exactly sure what we’re putting in our bodies, sometimes, depending upon what it is that we’ve purchased, and from what source, and what the company or group that’s put that together has put into that particular product.
Joe Saseen (guest): Very much so, and I think that’s an appropriate message to send to patients.
I will say that they’re, I don’t want to lead people to believe that all supplements are impure or bad. There are many reputable supplement companies that go through their own testing and put a stamp on the side of their bottle showing that they’ve went through good manufacturing processes and that they assure purity.
And for patients are using, let’s say, vitamin D to treat vitamin D deficiency or insufficiency. I would definitely want them, you know, they can use a supplement. But I would [00:06:00] direct them to one that has the stamp on the side that shows that they do own purity testing. Or somebody who’s using a multivitamin just for general, overall health. Or calcium for prevention of osteoporosis and those types of things. But those float into the vitamins and minerals versus the pure supplements.
Geralyn Warfield (host): So, as we’re thinking about our patients and their need to have some assistance sometimes in fighting inflammation, you talked a little bit about aspirin. You’ve talked about NSAIDs and some other medications.
Could you talk a little bit maybe about the mechanisms of action of some of those?
Joe Saseen (guest): Yeah. The, probably the easiest that everybody thinks about is aspirin and NSAIDs. Aspirin, when you use it in high doses, acts like an NSAID and an NSAID being something like ibuprofen or naproxen. And they simply work by being prostaglandin inhibitors.
So, they inhibit prostaglandins, which actually create inflammation. So, they inhibit the, I guess, in vivo process of developing [00:07:00] inflammation in inflammatory cells.
Some of the other therapies that we have, like colchicine…colchicine is very interesting because it is considered an anti-inflammatory drug in the treatment of rheumatologic conditions such as gout.
It works in microtubules, so it works very specifically in monocytes to actually decrease their activation and their propagation. Which, it’s a leap of faith, somehow to connect that to cardiovascular disease because it’s many steps downhill.
And we’re at the point where when we have these inflammatory treatments, we don’t always know how they may be associated with more or less cardiovascular risk.
And because we don’t know the exact pathway down there, it could be an association that risk goes down and inflammation goes down. So, it looks like the treatment, which is combating inflammation, is providing benefit when it may be some other explanation.
Geralyn Warfield (host): We’re going to take a quick break and we’ll be right back.
Geralyn Warfield (host): We’re back with Joe Saseen, talking about inflammation and cardiovascular disease. [00:08:00] And I’m wondering if you could please talk a little bit about the evidence about the medications that we’ve been discussing, be they aspirin, colchicine, anything in between or beyond.
Joe Saseen (guest): Yep. With aspirin, it primarily has efficacy when used in very low doses, which don’t even touch inflammation, that actually just produce anti-platelet effects.
And what we know is that for secondary prevention patients, absolutely they reduce cardiovascular events.
With primary prevention patients, there’s a small reduction in certain high-risk patients, but there’s also an increased risk of bleeding. So that’s sort of a plus/minus in primary prevention.
For NSAIDs, drugs like celecoxib, which is a pure COX-2 selective NSAID, or ibuprofen, or naproxen, we actually have proof that there’s an increase in cardiovascular events. For unknown reasons, it may be some interplay that when you’re inhibiting thromboxane a2 and prostacyclin, that there may be negating of the vasodilatory effects in coronary arteries that’s produced by the prostacyclin.
Maybe that [00:09:00] explains the result, which is an associated increased risk of cardiovascular events long term.
Short-term, I’m not so concerned with because the data really implies with persistent chronic long-term use, that’s where we see that increased risk. That’s why you have FDA labels that warn against that.
We have another drug, which is a common anti-inflammatory drug used for rheumatologic conditions like rheumatoid arthritis and other rheumatologic dermatologic conditions, which is methotrexate. And that definitely reduces inflammation. But when it’s been studied prospectively long term, it’s failed in the well designed prospective clinical trials to actually show reduction in cardiovascular events in high-risk patients. So that’s one that we know decreases inflammation, but it’s not associated with a decreased risk of cardiovascular events. So that’s an unknown.
We do, though, have another treatment, which is an anti-inflammatory called canakinumab. Canakinumab is a monoclonal antibody which targets interleukin-1 beta. An interleukin-1 beta is involved [00:10:00] with the propagation of the inflammation.
There’s one large trial called the CANTOS trial, which looked at the use of canakinumab at three different doses versus placebo in high-risk secondary prevention patients. And showed over a prolonged period of multiple years that there was a reduction in cardiovascular events with the 150 and 300 milligram dose.
So, it’s a proven treatment to reduce cardiovascular events in secondary prevention patients, but it’s offset by the increased risk of side effects. Serious side effects, such as serious infections, which are associated with immunosuppressive kind of picture with neutropenia and thrombocytopenia.
So that’s an example of one drug which has been proven to be effective in one trial, but has not hit primetime or recommendations because of it being one study and having an unbalanced risk-versus-benefit profile. It’s a treatment that we don’t see often used anyways, so it will lead to [00:11:00] further research using other anti-inflammatory drugs that are similar to that mechanism, which is blocking interleukin-1.
We also have a drug called colchicine, which is very, very old, used to treat acute gout, to prevent gout, and also for some other cardiovascular indications. And it has been studying two really big trials, prospective secondary prevention trials, looking at daily colchicine 0.5 milligrams once daily versus placebo. And in these two large trials, both of them showed a reduction in cardiovascular events.
So that’s very intriguing that we have an old drug that is available generically. That two large outcome trials have shown benefit, but we haven’t seen it used routinely in secondary prevention patients. Maybe because we have a milieu of other treatments to reduce cardiovascular events.
But we do have a guideline which should be released sometime in the near future from ACC and AHA, which is a guideline for treating patients who have chronic coronary disease. [00:12:00] And I am guessing that they will have a comment on that because of two large outcome trials. So that is a drug which is used for rheumatologic conditions and combats inflammation that’s proven to be effective, and maybe it’s another tool in our armamentarium to reduce cardiovascular risk in secondary prevention patients.
Geralyn Warfield (host): You have given us a lot to think about with all of these different opportunities for treatment for some of our patients. And we talked a little bit about the bleeding risk and other risk factors associated with some of these pharmacotherapies, and I’m wondering is there a go-to guideline or go-to resource that you would point our listeners towards to help us assess before, during, and after a clinical visit with a patient, you know, the benefit, cost, benefit analysis, if you will, of using these different pharmacotherapies with different patients?
Joe Saseen (guest): That’s a great question. I don’t know if there’s one collective resource. I do find personally, there’s probably ones I’m not aware of, but when I do go to [00:13:00] ACC, I actually go to their guidelines because they have cost value recommendations in a lot of their clinical guidelines. So, I do like that we have that available within guidelines produced by a cardiovascular organization.
There’s also, if you’re looking, it’s maybe not a tool, but it’s maybe an area. The ICER group does do cost-effective analyses, and they’ve published many of their findings. They’ve done analyses of bempedoic acid, they’ve done analyses with icosapent ethyl, which is an omega-3 fatty acid, used to reduce cardiovascular risk.
And they, while I’m not sure they have one tool available, they do have science and evidence that’s been produced, answering specific questions with certain drug therapies.
Geralyn Warfield (host): And is there anything else that you’d like to add that we haven’t had a chance to discuss?
Joe Saseen (guest): I guess what I’d like to add is when we think of cardiovascular risk reduction, it Incorporates so many different aspects of treatment. Everything from lipid management, hypertension [00:14:00] management, diabetes management, obesity management, smoking cessation, improving sleep, physical activity, and now perhaps even there’s an element of inflammation, that it can be overwhelming with the amount of treatment options and one package is not going to be applicable to every patient.
So, I think, I guess two messages I have is, one, make your decisions that are patient-centered and tailored using shared decision-making to what’s right for your individual patient. So, one size does not fit all.
And second is, hopefully you have access to resources, which are different professions that can work together collectively for this population.
Cardiovascular disease still is always remaining to be the number one cause of mortality in the United States. And the power of an interprofessional team that includes providers, medical providers, nursing providers, pharmacists, providers, behavioral health specialists, dieticians—the more professions you can have on your team to care for patients, the better the patient care is.
Geralyn Warfield (host): I think [00:15:00] the add-on that I would put into people’s heads is just that not only is it a team of healthcare professionals, it’s also the team of the patient, their family, the caregivers, and helping patients advocate for themselves, and where to find quality information about their disease state and all the other factors, I think is very important as well.
Joe Saseen (guest): Absolutely. Thank you for reminding me of that. The patient is always the center of the team, right? And is an important key member of that team.
Geralyn Warfield (host): Awesome.
Joe Saseen (guest): Including their caregivers.
Geralyn Warfield (host): Oh, most definitely.
Thank you so very much for spending time with us today. It’s been great to talk to you about inflammation and CVD and the interrelationships there.
My name is Geralyn Warfield. I am your host and I look forward to seeing you next time.
Thank you for listening to Heart to Heart Nurses. We invite you to visit pcna.net for clinical resources, continuing education, and much more.
Topics
- Atherosclerotic Cardiovascular Disease (ASCVD)
- Pharmacology
Published on
March 5, 2024
Listen on:

PharmD, FNLA, CLS
Related Resources
Online Interactive Guides
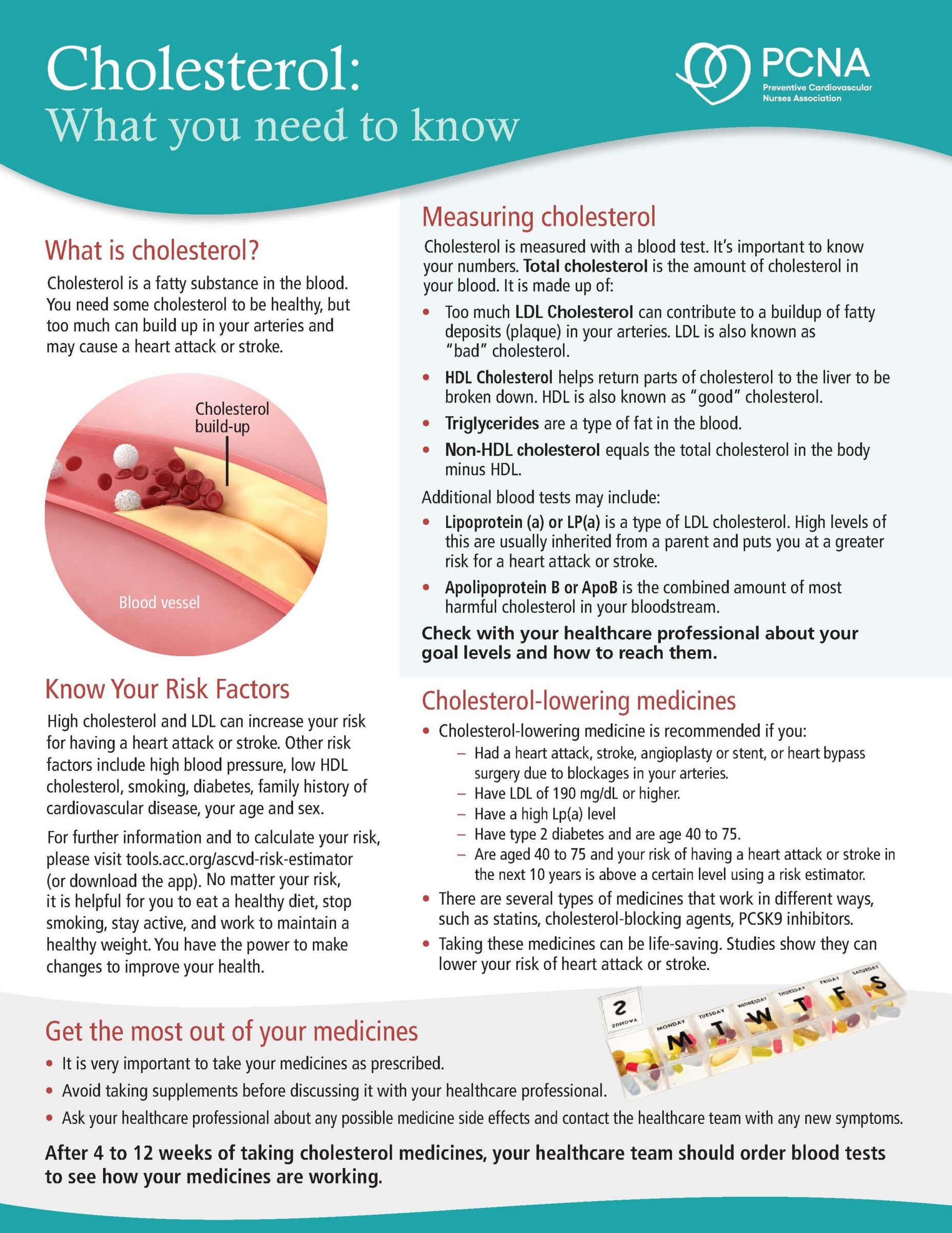
Cholesterol: Journey to a Healthier Lifestyle Online Interactive Patient Guide
February 12, 2025