One in two US adults has a hypertension diagnosis, yet not all hypertension is the same. Learn from guests Yvonne Commodore-Mensah, PhD, MHS, RN, and Ruth-Alma Turkson-Ocran, PhD, MPH, RN, FNP-BC, CNE, about primary/essential, secondary, and resistant hypertension, including the definition, diagnosis, and treatments, as well as the impact of non-adherence. Access to care, home versus clinic readings, and team-based care are also discussed.
This episode is supported by Medtronic.
Episode Resources
Renal Denervation #1 podcast episode transcript
[00:00:00] Welcome to Heart to Heart Nurses, brought to you by the Preventive Cardiovascular Nurses Association. PCNA’s mission is to promote nurses as leaders in cardiovascular disease prevention and management.
Geralyn Warfield (host): Welcome to today’s episode where we are going to be focusing on responsive versus resistant hypertension and novel treatment approaches. Today I’m so pleased to have with us Drs. Yvonne Commodore-Mensah and Ruth-Alma Turkson-Ocran. Dr. Commodore- Mensah, could you start us off by introducing yourself please?
Yvonne Commodore-Mensah (guest): Hello everyone. I’m Yvonne Commodore-Mensah. I’m an Associate Professor at the Johns Hopkins Schools of Nursing and Public Health. I’m also board member of PCNA. It’s good to be with you today.
Geralyn Warfield (host): We’re so glad to have you here, as well as Dr. Turkson-Ocran. Could you please introduce yourself to our [00:01:00] audience?
Ruth-Alma Turkson-Ocran (guest): Hi everyone. I am Ruth-Alma Turkson-Ocran. I’m a clinical investigator at Beth Israel Deaconess Medical Center and Instructor of Medicine at Harvard Medical School. I’m also a board-certified nurse practitioner. It is nice to meet you.
Geralyn Warfield (host): Thank you both for being here. We look forward to learning from you and exploring the interdisciplinary facets of our topics today.
To get us started, Dr. Commodore-Mensah, could you talk to us a little bit about ensuring that we’re all on the same page when it comes to primary hypertension?
Yvonne Commodore-Mensah (guest): So, primary hypertension, also called essential hypertension, is the most common cause of hypertension for most adults. There’s no identifiable cause of high blood pressure or hypertension.
So, this type of high blood pressure is called primary hypertension or essential hypertension. And according to the 2017 hypertension guidelines, 1 in 2 adults in the US has a hypertension diagnosis. But [00:02:00] we also know that there are pronounced disparities in the prevalence of hypertension in the US where about 57% of black adults have a hypertension diagnosis.
We also know that in some other racial and ethnic minority groups such as South Asians and other Hispanic groups in the US, there is also a high burden of hypertension.
But what is also concerning is that although there are evidence-based therapies to effectively control blood pressure, one of the concerning things is that although we know how to effectively manage hypertension, the prevalence of controlled blood pressure is low. Only 1 in 4 adults who are diagnosed with hypertension have the blood pressure controlled. And this is alarming because we know that hypertension is a leading risk factor for cardiovascular disease, [00:03:00] stroke, kidney disease, and is also linked with vascular dementia.
And so, I’m so glad that we are prioritizing this topic of hypertension and talking about ways to effectively manage hypertension and reduce the burden of hypertension in the population.
Geralyn Warfield (host): So, there’s a lot more to hypertension than just the primary hypertension that Dr. Commodore-Mensah described. And I’m hoping that you, Dr. Turkson-Ocran, could talk a little bit more about some other things that our clinicians that are listening to this need to be aware of when it comes to hypertension.
Ruth-Alma Turkson-Ocran (guest): So, in terms of, I guess, hypertension, a number of things that, we can consider is number one, the appropriate way to diagnose it. The fact that there are different types of hypertension including resistant hypertension, which I’ll get to talking to in just a little bit. But. [00:04:00] number one, to make a diagnosis of hypertension, you need at least 2 to 3 blood pressure readings, ideally taken on 2 separate visits.
We typically recommend that people use the 24-hour ambulatory blood pressure monitoring, or ABPM, to diagnose it. It’s considered the gold standard in making that hypertension diagnosis and also in diagnosing other patterns of blood pressure elevation, including hypertension, nocturnal hypertension, for example.
Whenever we see patients in, let’s say in the clinic setting, for example, and their blood pressure is not controlled, some of the things that we need to consider is what we are looking at resistant hypertension, for example. And, so resistant hypertension is, we can essentially define it as, blood pressure that remains above the goal for the particular person you’re interacting with, despite using at least 3 blood pressure medications at the same time.
And one of those blood pressure medications should be a diuretic. And each of these three different blood pressure medications should be in a different class of medication and should be at the highest tolerated dose, or at the most, at the highest tolerated [00:06:00] dose for that person. And then also at the appropriate dosing frequency for this person. And, I said that it remains above goal and the concept of being above goal can be different for different people depending on, maybe, the level of cardiovascular disease risk, for example, whether they have any other comorbidities.
And so, I would say that usually, and whether you’re measuring it using automated office blood pressure monitoring or ambulatory blood pressure monitoring, for example. And so, usually it’s above. I would say, you know, at least between 120 to 130 for systolic and about 80 for diastolic, again, depending on what, how, you’re measuring it and what the person’s cardiovascular disease risk is.
However, I want to say one thing, especially [00:07:00] since Dr. Commodore-Mensah talked about controlled hypertension, about a hypertension that’s controlled, is that we can still have people who are taking 4 or more anti-hypertensive medications and have controlled blood pressure.
For people who are on those 4or more anti-hypertensive medications, and their blood pressure is controlled, we’ll still call them, I also categorize them as having controlled resistant hypertension. And I’m hoping that we can get more into the statistics here about resistant hypertension.
And one of the things that we see is that it’s pretty, we usually see it among young, we see it among the adult spectrum, but we see a little bit more among [00:08:00] adults or I guess adults between age ages 18 to 40 years old.
But, to also make the one thing that we want to know is that to make the diagnosis of resistant hypertension, you also want to make sure that you’re excluding other types of, you know, what we call pseudo resistance of blood pressure. So, for example, things that are making it appear for you in the clinic setting that someone has an uncontrolled, high blood pressure.
And so, you want to exclude things like non-adherence for medications, for example, but also other types of blood pressure–I’ll call them phenotypes. For example, are they experiencing the white coat effect? And, to do that, it’s important to [00:09:00] examine what is blood pressure doing, not only in the clinic setting when you’re seeing patients, but also out of clinic setting.
And so, using things like 24-hour ambulatory blood pressure monitoring to assess for does the person have white coat effect. White coat effect is contrary to white coat hypertension, is when someone is still treated and high on high blood pressure medications, but you’re still seeing an elevation of blood pressure in the clinic as opposed to out of the clinic.
Do they have nocturnal, you know, high blood pressure? Are they taking the medications at the dosing that you’re telling them to take them at the timing that they’re expected to take them? And, I know Dr. Commodore-Mensah, I know you do have a little bit more to say about blood pressure measurements outside the clinic setting.
Yvonne Commodore-Mensah (guest): In terms of diagnosis of resistant hypertension, it’s also [00:10:00] important to consider the issue of medication non-adherence as one of the potential challenges. So, in a case where a clinician may suspect resistant hypertension, it may be that there’s an issue with medication non-adherence.
And so, this is a very complex issue because, as clinicians we may be tempted to blame the patients for not being adherent to their treatment. But we know that there are multiple determinants of non-adherence to antihypertensive therapy. For instance, is a patient not tolerating the medication? Is it possible that they can’t afford the medication?
So, it’s an important to assess and address medication non-adherence in a non-judgmental manner, and ask the right questions about, patient’s medication-taking behavior to understand whether blood pressure control was not achieved because [00:11:00] of issues surrounding medication adherence.
But we actually know that in patients who are diagnosed with hypertension, some estimates suggest that 50 to 80% of them are not adherent to their therapy. So, it turns out that this is an issue. In many cases it may be medication non-adherence rather than resistant hypertension. So, once we rule out this issue and ensure that indeed patients are taking the medications as prescribed, and blood pressure control is not achieved, and we rule out the white coat effect that Dr. Turkson-Ocran mentioned earlier, then we can start to think about whether this may be indeed, resistant hypertension.
Ruth-Alma Turkson-Ocran (guest): I would also like to add that in addition to resistant hypertension, we also have to consider other reasons for the elevated blood pressure that is [00:12:00] not under control.
And that is where we can come to, I guess, secondary hypertension. So, we already talked about, you know, primary hypertension. We don’t necessarily know why that may be happening. But then secondary hypertension is that, you know, people’s blood pressure may be uncontrolled, when we are interacting with them or above goal, like I prefer to say, above goal versus uncontrolled, so, above the goal that you have set with them.
And so, when we are looking at the whole clinical picture, oftentimes then we may see clinical clues that may, you know, tease the fact that maybe there’s something else that might be going on that may be influencing their blood pressure, making elevated and for these persons, unlike the [00:13:00] persons who have essential hypertension, primary hypertension.
We need to be sleuths and go digging a little bit deeper to see what exactly could be causing these elevations in blood pressure. Because some of the reasons why they may be having elevated blood pressure, some of the reasons for this, that elevation can be addressed, can be maybe even cured, leading to improved blood pressure measures and even maybe even getting into the whole normal blood pressure range.
And so, there, I guess we can consider some of these factors and consider that some of them may be what we call due to renal vascular disease.
So, for example, especially those that are caused by atherosclerosis, so it may be atherosclerosis of the coronary arteries [00:14:00] or even peripheral arteries.
And some of what we consider with the peripheral includes renal artery stenosis, or/and maybe especially maybe in younger women, we may also consider fibromuscular dysplasia. So, some of these things, some of these clues are maybe, you start them, and I know we’ll be talking about medications in a little bit. So, making a plug for that.
So, you may start them on a medication, for example, maybe an ACE inhibitor or an ARB (an angiotensin receptor blocker). And, after about, you know, so you always want to do lab work, and you see a bump in the maybe serum creatinine, for example, about 50%. That might be a clue to you to say, “Okay, what exactly is going on?”
You may also, so in addition to renal vascular disease, we may also think about what about primary renal disease that may be causing the [00:15:00] elevations in blood pressure. So, here’s where we, again, we see elevated, serum creatinine or eGFR elevations. Do they have, primary aldosteronism, for example? And some of the clues that you may see with this is that, you know, maybe is their potassium off? So, are they having hypokalemia? And so, we see that very, very commonly. And so, you may just want to think that, okay, is it being caused maybe by an adrenal adenoma, is it being caused by something else?
So, whenever we see, hypokalemia, usually due to the urinary excretion of potassium, that’s one of the things that we want to think about. Do they have hypoaldosteronism? And it’s one of the, actually, really common causes of drug resistant [00:16:00] hypertension. So, then you want to do a urinary potassium test, for that, or you want to look at the ratio of aldosterone reading and aldosterone ratio. So, you want to look at that.
But, to do those tests, there’s other things that you want to do. Sometimes they may be on medications that may be affecting the renal aldosterone ratio. So, you want to hold those for about 4 weeks. So, some of those medications could include things like NSAIDs, for example. And spironolactone a MRA—mineral corticoid receptor agonist. That’s a little hard to say. So, something like, spironolactone or eplerenone. So, are they on those kinds of medications? Are they maybe even taking licorice? People don’t think about that. Are they on any other potassium wasting diuretics, for example.
The other causes of secondary hypertension, really common, is are they taking medications that may be leading [00:17:00] to higher blood pressure? So, we have, several different medications. I talked about NSAID, for example. Are they taking oral combination, oral contraceptives or those with estrogen in them? Are they taking stimulant, you know, whether it’s coffee, whether it’s for weight management, for example? Are they taking, and some antidepressants also cause that, as well as chemotherapy medications. There are so many, even antifungal medications like Ketoconazole, for example, can also cause.
So those are really, really common medications. Then we need to look at, okay, are they having sleep apnea? And so, one of the things that you want to do is always, always screen for sleep apnea. Do the STOP BANG because people who have sleep apnea, they usually would retain some sodium and then not respond as well to [00:18:00] anti-hypertensive medication.
Geralyn Warfield (host): Our guests have really given us a lot to think about already when it comes to hypertension. We’re going to take a quick break and resume our conversation in just a moment.
Geralyn Warfield (host): We’re back to continue our discussion about resistant hypertension with Drs. Commodore-Mensah and Turkson-Ocran. We know from a larger clinical perspective that social determinants of health have an impact on our patients as well as our practice.
How specifically does this affect hypertension diagnosis and treatment?
Yvonne Commodore-Mensah (guest): That’s an excellent point, Geralyn. We know that when it comes to disparities in hypertension diagnosis, treatment, and control, like I said earlier, there are pronounced disparities along racial and ethnic lines, but there’s also greater recognition that the underlying cause of these disparities is what we call social determinants of health—so, the conditions in which people learn, play, work, or pray which [00:19:00] may affect, their overall health.
So, when it comes to hypertension treatment, diagnosis and control, we must consider what are some of these circumstances that may get in the way of people being screened for hypertension, receiving appropriate treatment, but also having the blood pressure control.
One of the most important factors is healthcare access. We know that although there have been efforts to improve healthcare access in the US with fewer Americans being considered uninsured, we also know that we have this issue of under insurance. Even for those who may have health insurance, they still may have limited access to primary care providers. So, in some instances, people may have to wait months to be seen by a provider, and if they have a health-related [00:20:00] question, they may not have access to a healthcare provider. And so, healthcare access is one of the challenges that we should consider when we think about why blood pressure control is not obtained or achieved.
So, one of the strategies is to ensure that we’re providing multiple opportunities for people to be screened/diagnosed with hypertension. So, in terms of screening, we need to consider how we may engage with communities, underserved communities, to screen for hypertension. How may we partner with community-based organizations, faith-based settings? And this is where nurses can play a really instrumental role in partnering with organizations to be more present and visible in communities to screen people for hypertension, to provide education regarding the causes of hypertension, how to effectively manage and control hypertension.
And so, these are opportunities that we [00:21:00] can take advantage of collectively to try to reduce the burden of hypertension. When it also comes to treatment, I mentioned earlier that medication non-adherence is also an issue. So, we must also consider what are some of the reasons why people may not be taking their medications as prescribed.
There are individuals who may have insurance, but they may still have to pay out of pocket for certain medications, which may get in the way of them deciding to take their medications appropriately. I actually recall in one of our community-based screenings, I met a participant and we started talking about her blood pressure, which was elevated at that time.
And then she admitted to me that she skipped her medication because she didn’t have enough. She couldn’t afford her medications. So that’s a concrete example of why we may see a patient in a clinical or community setting, and they may have uncontrolled hypertension, and it may [00:22:00] not be that they willingly decide not to take their medication; it’s just that in some cases they may not be able to afford their medication. So, we need to work together to make sure that everyone has access to medications, to control blood pressure.
And also, in terms of considering solutions, reducing the amount of copay or making antihypertensive therapy free, especially for high-risk patients who may have issues affording these medications is another solution we can consider.
So how may nurses be strong advocates for, improving healthcare access and making medications more affordable for all our patients? Earlier Dr. Turkson-Ocran talked about the importance of out-of-office blood pressure measurement to rule out resistant hypertension. And so, we also need to consider how we can ensure that for patients who are diagnosed with [00:23:00] hypertension, that they have access to home blood pressure devices that are validated but are also affordable.
These home blood pressure devices support our patients in self-management of their blood pressure. I’ve seen it with my own eyes in terms of engaging with people in the community, who, when they have a blood pressure device at home, they’re able to tell how changes in their behaviors or their medication adherence may impact their blood pressure.
So, as we talk about effectively diagnosing hypertension and managing hypertension, we need to ensure that all patients have access to these validated blood pressure devices as well.
Geralyn Warfield (host): Now that we understand more about hypertension and how it is impacted by the social determinants of health, let’s pivot to treatment options.
Dr. Commodore-Mensah, could you start us off talking with our audience about treatments?
Yvonne Commodore-Mensah (guest): One of the mainstays when it comes to blood pressure control or management is [00:24:00] lifestyle modification. I think we know that there are effective anti-hypertensive medications, but lifestyle management should be a cornerstone of controlling hypertension.
I like to say when I engage with people in the community that food is medicine, exercise is medicine. And as we think about ways to improved blood pressure control, we need to emphasize the importance of lifestyle changes. So, we know that food patterns, that allow people to lose weight if they have obesity, have been shown to lower blood pressure.
We also know that a diet that is lower in sodium may also help to lower blood pressure. We also know that physical activity, so, being active, also helps to improve blood pressure control. And when you think about the additive effects of losing weight, if someone has obesity, being [00:25:00] physically active, but also adopting a dietary pattern that is consistent with, for instance, what we call the DASH diet. So, DASH stands for Dietary Approaches to Stop Hypertension. So, this is a diet that is high in fruits and vegetables and low in saturated fats. So, that diet has been shown to help lower blood pressure.
So, as we talked about blood pressure controls, it is important to first bring up that conversation that what can patients do to control blood pressure in addition to taking their medications that’s prescribed.
But we also need to consider that unfortunately, for some patients, they may not have access to these foods and vegetables that may allow them to improve their blood pressure. And for some patients, they may not live in environments that may allow them to be physically active. And that’s why it’s important that as we talk about lifestyle modification, we think [00:26:00] about assessing and addressing social determinants of health so that we are aware of some of the barriers that may get in the way of patients adhering to some of these lifestyle recommendations as well.
But I’ll turn it over to my colleague, Dr. Turkson-Ocran, who may also have some insights on lifestyle modification.
Ruth-Alma Turkson-Ocran (guest): Right. I think to add to lifestyle modification, I think one thing that we may often under-emphasize is also moderation in alcohol use.
Because we know we’ve seen the effects of alcohol in elevating blood pressure. But also, I would also like to put the plug, in addition to the DASH eating pattern. also consider the use of, and lowering sodium, but also the use of sodium of substitutes. And so, we know that a [00:27:00] diet, an eating pattern, I don’t like to call the DASH diet dash a diet, but eating pattern that is lower in sodium but also higher in potassium. essentially lowers blood pressure. And the sodium replacement also essentially either reduces [or replaces] the levels of sodium in what we eat.
So, whether you’re maybe starting off with a maybe a 50/50 replacement, and then moving on to maybe a 70/30 replacement, and then full sodium replacement with potassium, those we’ve also seen, because, you know, potassium tastes exactly like salt. We’ve also seen, really an improvement in people’s blood pressure with that. But we also want to make sure that we’re, monitoring their labs—particularly potassium—because we do have a very [00:28:00] narrow therapeutic window for potassium.
Geralyn Warfield (host): And what about other treatments beyond diet, exercise, and lifestyle?
Ruth-Alma Turkson-Ocran (guest): So, I usually see that, you know, lifestyle modifications are the first-line therapy. But then when we talk about going into medication, for example, we consider essentially the following as the first line medication therapy for hypertension.
And so, you want to start out with a thiazide or a thiazide-like diuretic. So, for example, we’ve more in the maybe recent past used a lot of hydrochlorothiazide, but there are also other, much longer-acting, and frankly preferred, thiazide diuretics. For example, chlorthalidone or indapamide, for example.
So, for me, in my practice, I’m usually trying to switch people away from hydrochlorothiazide, which is [00:29:00] shorter-acting into the longer-acting chlorthalidone or indapamide. And so then, the second one is, are we looking at an ACE inhibitor, an angiotensin converting enzyme inhibitor, or an angiotensin receptor blocker.
So, things that would maybe be considered, ACE inhibitor medications that may be considered…ACE inhibitors include enalapril, lisinopril. And then those that are ARBs usually end with “-sartan”: candesartan, losartan, valsartan, things like that. And then the third class of medications that are also considered first-line: calcium channel blockers. So, you have the main ones that we use which are amlodipine and nifedipine.
And so, these three: thiazide or thiazide-like diuretics, ACE [00:30:00] inhibitors, or ARBs or calcium channel blockers, those are the first-line medications you want to start people on when you’re starting a blood pressure medication.
And then we move on. So then, I guess maybe going back to the discussion about resistant hypertension, you know, given that we know that the most common causes of secondary hypertension include, you know, things like renal artery stenosis, chronic kidney disease, sleep apnea and primary, hyper primary aldosterone, we can also work towards, you know, addressing those kinds of issues. So, for example, we can use MRA or mineral corticoid receptor agonist. Things. I think I mentioned them earlier: spironolactone or eplerenone, [00:31:00] are also helpful for people who have primary hyperaldosteronism, to just help with their blood pressures.
Then once we are moving on, we can go into medications like beta blockers. A lot of times, [00:32:00] again, beta blockers are not first-line, but we also use them as adjuncts, especially if maybe they might be having maybe side effects of some of the other medications. Sometimes the beta blockers can help, with, I guess combat, some of the side effects that they may have.
And then we move into other medications that we don’t necessarily prescribe that often, for example, clonidine. So, you take clonidine 2 to 3 times a day. We usually prefer the patch actually. You also have other medications or vasodilators. So, for example, hydralazine and minoxidil.
Again, you’re going into [00:33:00] I guess deeper waters with that, but in all of these things we want to make sure that we are just taking a multidisciplinary approach. And so, whether, as nurses, as nurse practitioners, we want to work with other members of the team, whether it’s endocrinologists, nephrologists, cardiologists, pharmacists.
So, in our hypertension clinic, we have pharmacists that actually see patients. Also, we want to work with community health workers, dieticians, social workers, and even psychologists also. Addressing resistant hypertension in all these different ways.
And then, we also moving into, I guess what for us here in the US is [00:34:00] maybe newer therapies. Some of them include the longer-acting injectable medications, but also renal denervation. And it’s something that we’re going to be talking about in our subsequent podcast.
And so, it’s newer and FDA-approved more recently here in the US. In Europe it’s been done for a few more, longer, years but we will be talking about that. And there’s been a lot of clinical trials that have been found finding that denervation has been effective.
And so, those are several different [00:36:00] options or therapies that we use for people who have resistant hypertension, refractory hypertension.
I think a lot of times we also, in discussing the approaches for the general public, we also tend to leave out people who have a uterus who may be in a childbearing age, who may become pregnant, and what are therapies that we have for them. And so, we know that we cannot, or we don’t want to , treat their hypertension with ACE inhibitors, ARBs, or direct renin inhibitors due to the impact that it can have on fetuses.
And so, for those who end up, who are planning to become pregnant, who become pregnant, you want to transition them to medications like methyldopa, the extended-release nifedipine, labetalol during pregnancy. And there are [00:37:00] also treatment goals for pregnancy, we want the systolic to be less than 140, and diastolic less than 90.
So didn’t want to leave out this group of people when we’re talking about treatment for hypertension and medication for hypertension. These are things that we also want to be considerate about.
Geralyn Warfield (host): I have a final question for each of you, and that would be what would be the top takeaway for our listeners about today’s topic of resistant hypertension?
Dr. Commodore-Mensah, I’m going to start with you.
Yvonne Commodore-Mensah (guest): For me, a good takeaway would be to consider other more plausible causes of what would be considered resistant hypertension. And that would be assessing and addressing medication non-adherence. So, understanding from the patient’s perspective, what are their medication-taking behaviors.
Are they able to afford their medications? Are they experiencing side effects? [00:38:00] When we’ve addressed some of these issues and blood pressure control is not achieved, then we can think about other reasons such as resistant hypertension, but unfortunately, for the large majority of our patients, blood pressure control is not achieved for reasons that we’ve discussed so far.
And we also know how to treat and control hypertension. The evidence is clear that team-based care, home blood pressure monitoring, treatment intensification, those are all evidence-based strategies to effectively control hypertension. So, even as we have these novel therapies, we also need to consider how some of these novel therapies may be available or accessible to the people who need it the most. And ensuring that they are affordable so that the [00:39:00] individuals who are higher risk for complications from uncontrolled hypertension also have access to these novel therapies as well.
Ruth-Alma Turkson-Ocran (guest): I guess one of the things that I would add, and I think Dr. Commodore-Mensah actually said, some of the stuff that I was thinking is that, but I’m going to expand just slightly on it, is the importance of self-monitoring blood pressure, or essentially taking, some aspect of taking control of some aspect of our treatment.
And, and that is engaging in, again, using a validated…getting a validated home blood pressure monitor and then monitoring your blood pressures. Because I think as people, we don’t know when and where we may get into [00:40:00] contact with the healthcare setting and under what circumstances.
And so, if someone is checking their blood pressures at home on a regular basis, a lot of times we recommend that you check your blood pressure, there are those steps in which we want you to check your blood pressure. So, your feet flat on the ground, your back supported, shouldn’t have the urge to—you should have emptied your bladder, not consumed any kind of, for example, coffee or anything that would impact your blood pressure about 30 minutes before your blood pressure, and then supporting your arm. It is important using the important steps and you can target BP has all those steps.
And so, measuring your blood pressure appropriately, using the correct technique, also when you measure it, wait about a minute and then measure it again. So doing it in duplicate, [00:41:00] at least twice a day. At the very least, you can have three times a week. We’ll take much more than that but then knowing what your blood pressure trends are, so you can tell if your blood pressures are trending upward or they’re trending lower, and maybe you’re having certain symptoms.
That way, you can let your clinician that you’re working with know. But also if you’re in a setting where maybe your blood pressure is due to stress, maybe an inappropriate measurement came out higher than your trends are usually at home, you can say “I have evidence that my blood pressures are good at home, that my blood pressures are controlled and maybe this is abnormal because of stress, because of improper technique, or something like that.”
Because we are not always as clinicians going to be with you at home, outside the clinic setting. So just kind of emphasizing the importance of home blood pressure monitoring, [00:42:00] blood pressure monitoring using the correct technique, monitoring trends and coming to us, the clinicians, when things, are not going how they usually are for you.
Geralyn Warfield (host): We are so appreciative to our guests today, Drs. Commodore- Mensah and Turkson-Ocran, for sharing their expertise about hypertension with our listeners.
We have spoken about a lot of different topics today, and you’re going to find some more information about those in our show notes for this episode. You can also find more information at pcna.net.
We are looking forward to our next episode where we’re going to spend a little bit more time discussing renal denervation in detail, so we invite you back to listen to that episode.
We’d also like to thank Medtronic for the support of this particular episode.
This is your host, Geralyn Warfield, and we will see you next time.
Thank you for listening to Heart to Heart Nurses. We invite you to visit pcna.net for clinical resources, continuing education, and much more.
Topics
- Atherosclerotic Cardiovascular Disease (ASCVD)
- Hypertension
Published on
April 16, 2024
Listen on:

PhD, MHS, RN, FAAN, FAHA, FPCNA

PhD, MPH, RN, FNP-BC, CNE
Related Resources
Online Interactive Guides
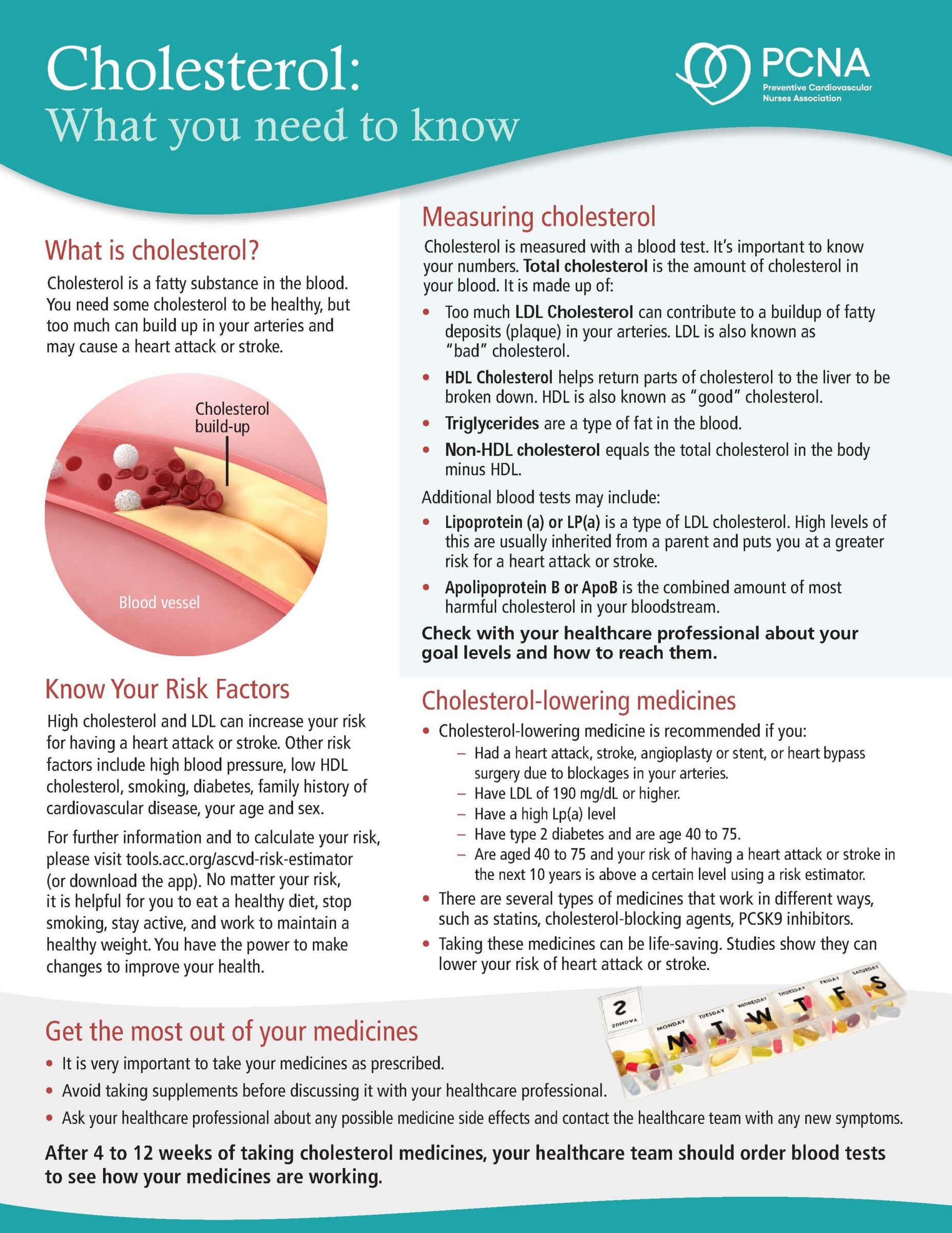
Cholesterol: Journey to a Healthier Lifestyle Online Interactive Patient Guide
February 12, 2025