What are some effective strategies for transitions of care for patients in acute-care settings? Guests Jessica Bell, BSN, RN, CCRN, and Kimberly Martinez, DNP, RN, CCRN, discuss starting education early, working as a team to layer information, and engaging family members and others in the process.
Episode Resources
- PCNA Patient Tools:
Welcome to Heart to Heart Nurses, brought to you by the Preventive Cardiovascular Nurses Association. PCNA’s Mission is to promote nurses as leaders in cardiovascular disease prevention and management.
Geralyn Warfield (host): I’d like to welcome our audience today to our episode where we have two incredible guests who are going to talk us through a little bit about the trajectory of patients from emergency room to back home. And I’m going to turn it over to them to introduce themselves. Kim, would you like to get us started?
Kimberly Martinez (Guest): Sure. my name’s. Kimberly Martinez. I am a nurse manager at UF Health in Gainesville, Florida, and I’m a nurse manager on a cardiovascular step-down unit.
Geralyn Warfield (host): Perfect. And how about you?
Jessica Bell (Guest): My name’s Jessica Bell. I am also a nurse manager at UF Health Shands in Gainesville. I manage the cardiology ICU.
Geralyn Warfield (host): So, Jessica, [00:01:00] could you start us off with the patient journey at your facility because you have a unique perspective in terms of how you see them first.
So, in what capacity do you see them and where do they go next?
Jessica Bell (Guest): Sure. So, at UF Health Shands—and probably most institutions around the nation—we see patients in our ICU facility that have come straight from the ED, the cath lab, some sort of emergent situation where they need that higher level of care.
And then after they’re done with us, they transition over to Kim’s unit or step-down unit. But like most places we sort of start that transition of discharge, that transition of care, from the very get-go from when they first sort of stepped foot on my unit.
Geralyn Warfield (host): And what does that look like when they get to you then Kim?
Kimberly Martinez (Guest): They come from Jessica’s unit. Primarily would be the cardiac teaching service, which is MI patients, [00:02:00] patients that have very recently had an MI. And they have very brief hospital stays.
And then we have heart failure patients, which can have much more lengthy stays and they can bounce back and forth between our two units. But those are the two patient populations that we see mostly.
Geralyn Warfield (host): So, there’s a great interplay for the two of you in terms of the information that’s shared at all those levels plus talking about meds. I mean, these are pretty significant changes in people’s lives. And so, what can you tell me a little bit about the education that happens in both of those locations?
Kimberly Martinez (Guest): Absolutely. The education is very important. the patient population that has just suffered an MI, they have a very traumatic, stressful event happen in their life, and then they have a very brief hospital stay and we want to get them back home. So, in that short time, we need to set them up and educate them so that they successfully go home and stay healthy.
The heart failure [00:03:00] population, that’s a terminal diagnosis. And their quality of life is what we really focus on then. We want to keep them out of the hospital. We want to keep them home, having activities with family. We want to extend their life as much as possible. So, we do a lot of education with them about watching their weight, fluid intake, when to notify the doctor.
Geralyn Warfield (host): So, in practice, what does this look like? You gave me an intriguing statistic about how much time your patients spend with you when they are the MI patients. If you could tell our audience about that and then maybe describe for us what that education looks like. Is that intensive during a big block of time? Is this happening throughout? What does it look like?
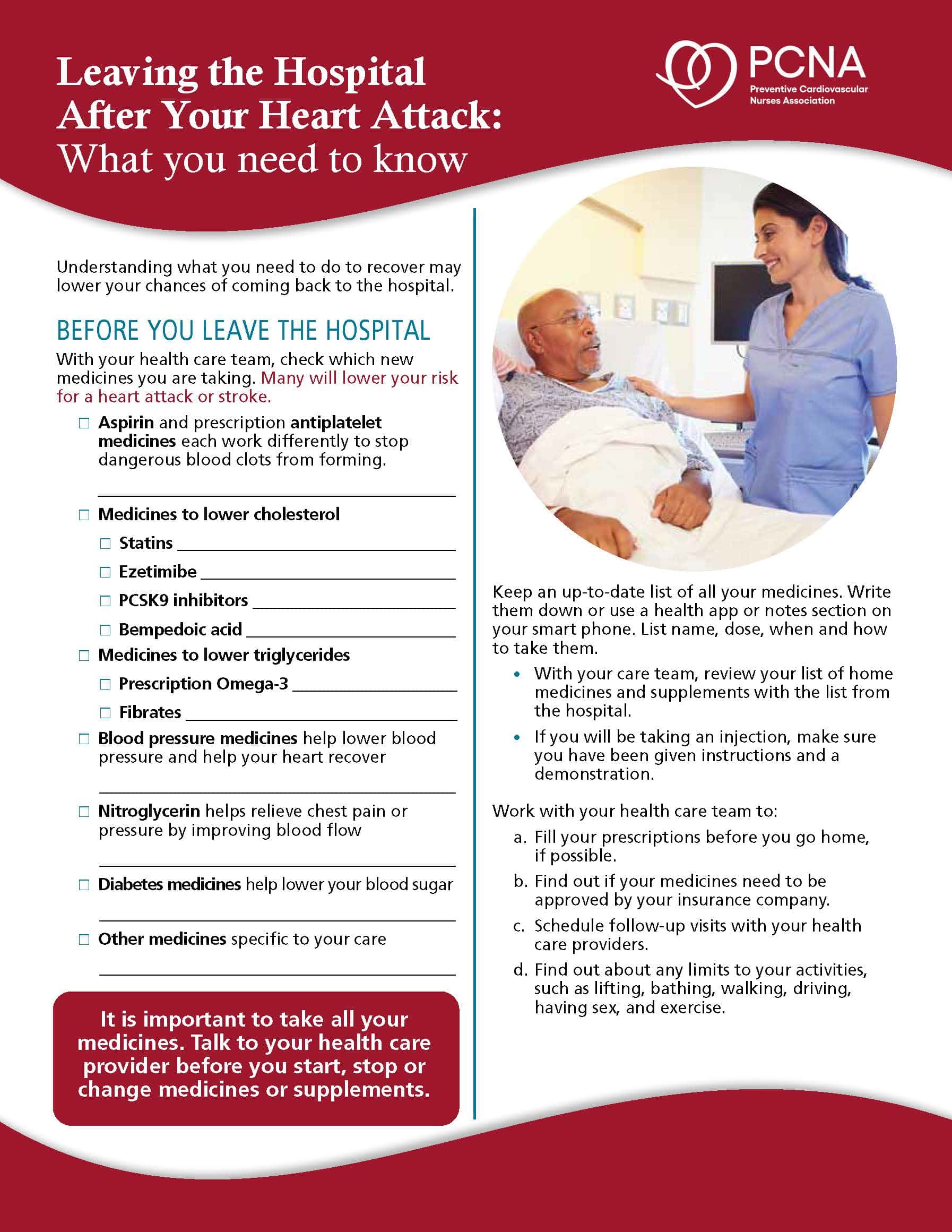
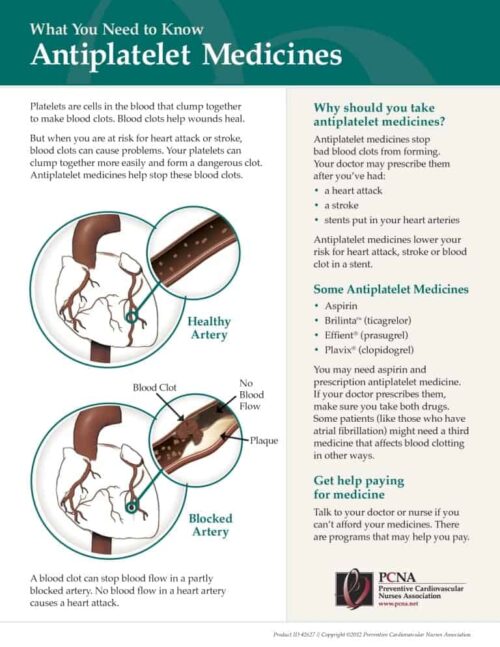
Kimberly Martinez (Guest): It happens throughout, but we only have a little bit of time while in the hospital. So, it’s important that we hit on some key points, primarily educating about the importance of taking anticoagulant medication immediately on discharge and continuing that medication. Because it’s such a short amount of time and [00:04:00] that patient’s still in shock usually, what follows afterwards is very important.
Jessica Bell (Guest): Yeah. And I think that that really does start in our acute care setting, right? Whether it’s my unit or Kim’s unit. The patient could be, you know, fresh into the ICU and our team is already starting those conversations. Our case managers are already working on what that discharge is going to look like, so that we can set these patients up to succeed and stay out of the hospital.
And I think Kim’s team really does a great job of just continuing that education as that immediate, you know, post-shock event has happened. And they’re kind of going, “OK, this is going to be what my life is like next.”
And so, we really partner not only with our med surg units, our step-down unit to take care of some of that education piece, but we also partner with our case managers, our social workers, our physicians, to make sure that all of those boxes are really checked.
Geralyn Warfield (host): And are you finding that that education is also happening with [00:05:00] the family or the caregiver in the room or at bedside as well?
Jessica Bell (Guest): Preferably.
Kimberly Martinez (Guest): Yeah, preferably. Jessica and I are both on the policy team for our partners in care policy; we’ve recently changed the name of it from a visitor policy because of how important the chosen person or people of the patient are in their recovery.
Jessica Bell (Guest): Yeah. And we really do, we partner with whomever that patient is identified as their partners in care to just make sure that we’re including them from the very beginning. Because we all know that it’s going to be their key to success. The patient’s key to success is going to be how well we can partner with their loved ones.
Kimberly Martinez (Guest): Especially with that messaging and education. Sometimes, the patient’s not ready to hear, they’re not in that accepting of education mind frame. So, having that patient family member hear that, it’s invaluable. As well as the [00:06:00] advocacy. So, just being able to vocalize what that patient might need, that the patient’s unable to do themselves.
Jessica Bell (Guest): Absolutely.
Geralyn Warfield (host): We are going to take a quick break and we will be right back.
Geralyn Warfield (host): We’re back with our discussion in terms of a patient transition of care from an acute event, an acute event I should say, like MI or diagnosis of heart failure as examples and what that transition looks like within the acute care setting.
But one of the things that I think your team has expertise in from which all of us could learn is what does that transition of care then look like as they’re leaving your facility? How do we set them up for success when they’re not sitting with you at bedside or, you know, wherever they are learning from your team?
I think you’ve got a great model in terms of engaging different parts of your community in that process. What does that look like?
Jessica Bell (Guest): Yeah, we really do. We have, really partnered with our, case managers to make sure that we [00:07:00] have all of those boxes checked, like I mentioned earlier, just to make sure that the patients are leaving and they’re leaving with all the tools that they need.
So, we work really hard with our case managers to make sure that that, you know, no matter who’s covering, the right things are getting ordered for the patient. And so, they do have a physical checklist. Our physicians have a physical checklist that’s posted in their workroom.
So, we make sure we have everything kind of addressed before discharge. We’ll make sure that they have a clinic visit. So, we have a post-MI clinic that their patients will see if they’re a post-MI. We make sure that they’re set up with meds to beds, which is delivery of medications before the patient leaves the hospital. So, they leave with all of those important medications in hand before they’re discharged.
We get them set up for cardiac rehab. We make sure that they are leaving with all their home health care needs and tools. So, if it’s a heart failure patient, they’re leaving with a little heart failure kit. [00:08:00] If it’s somebody who needs home healthcare, that’s already set up and ready before the patient’s out the door.
Geralyn Warfield (host): Are there any other strategies that you would share with the listeners in terms of other nuggets of success, that you think they’d like to know?
Kimberly Martinez (Guest): Sure. I think I’d like to expand on the MI clinic a little bit because that’s something we’re really proud of. Jessica can speak to this a little better, but I’ll set you up.
So, every Friday there’s a MI clinic and, the patients go when they see a few very key personnel to ensure that they are going to have success.
Jessica Bell (Guest): Absolutely. So, our MI clinic runs every Friday. So, if a patient were admitted Monday through Thursday, for an MI—if they were discharged in that timeframe, I should say—then hey would be seen that following Friday.
If it were a Thursday or a Friday, they would be on the next week they would be seen by a [00:09:00] cardiologist, a pharmacist, and our cardiac rehab. So, it’s a clinic that just consistently runs that day, and we make sure that every patient touches those three key people.
So, they’ll meet with a cardiologist. It’s probably not their primary care cardiologist, but it is a cardiologist who can address any acute issues, make sure that there’s anything that needs to be addressed is addressed. That cardiologist believes that that patient needs to be seen quicker than their scheduled visit, then they will reschedule that visit with their primary cardiologist.
The pharmacist will go over all the medications, make sure that affordability isn’t an issue, make sure that they have access to medications and just any other like hiccup that might have come from discharge.
And then the cardiac rehab team will see them as well. Introduction to cardiac rehab: let them know what the importance of cardiac rehab, what the expectations are going to [00:10:00] be of cardiac rehab. We see a lot of patients in our hospital, in our facility, that don’t necessarily live in our town. And so, sometimes we may have set them up with cardiac rehab with us. And that’s just not feasible, right?
So, that specialist at that time will find somebody closer to them and kind of get them set up with the right people so that we can assure that the patients are getting all of the care that they need post-discharge to keep them out of the hospital.
Geralyn Warfield (host): Is there anything else that either of you would like to add that we haven’t talked about already?
Kimberly Martinez (Guest): I would just like to emphasize the importance of all of the collaborators in patient care—the collaborative team, the nature of our team from inpatient, outpatient. All of those play a role in the patient’s journey through the healthcare system.
Geralyn Warfield (host): It’s obvious to me and probably to our audience, how much care and consideration has gone into the planning and now the execution of these plans [00:11:00] for these patients and how you do set up those patients and their families for success.
So, thank you very much for sharing your expertise, for your gems and wisdom. We really appreciate it, Jessica and Kim. Thank you so very much for being here.
I’m Geralyn Warfield, your host, and we will see you next time.
Topics
- Acute Coronary Syndrome (ACS)
- Heart Failure
Published on
October 1, 2024
Listen on:

BSN, RN, CCRN

DNP, RN, CCRN
Related Resources