Familial hypercholesterolemia (FH) affects 1 in 250 individuals, and genetic testing for patients and families is an important part of diagnosis and management. Guest Seth Martin, MD, reviews FH risk factors, at what ages and when genetic testing is recommended, and the roles of a genetic counselor and other team members.
Episode Resources
- NLA Statement on Genetic Testing
- FH Diagnosis
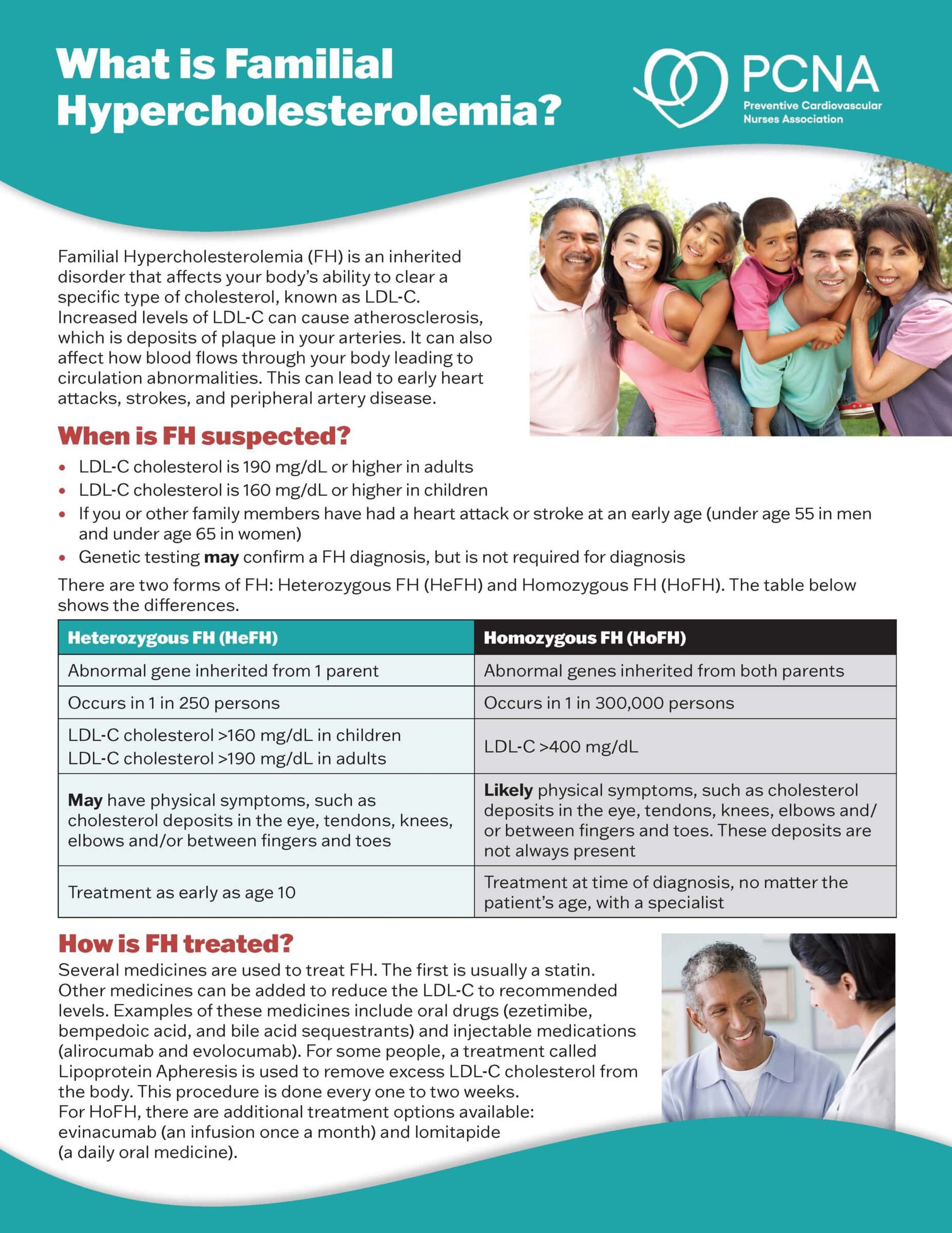
- What is Familial Hypercholesterolemia patient fact sheet
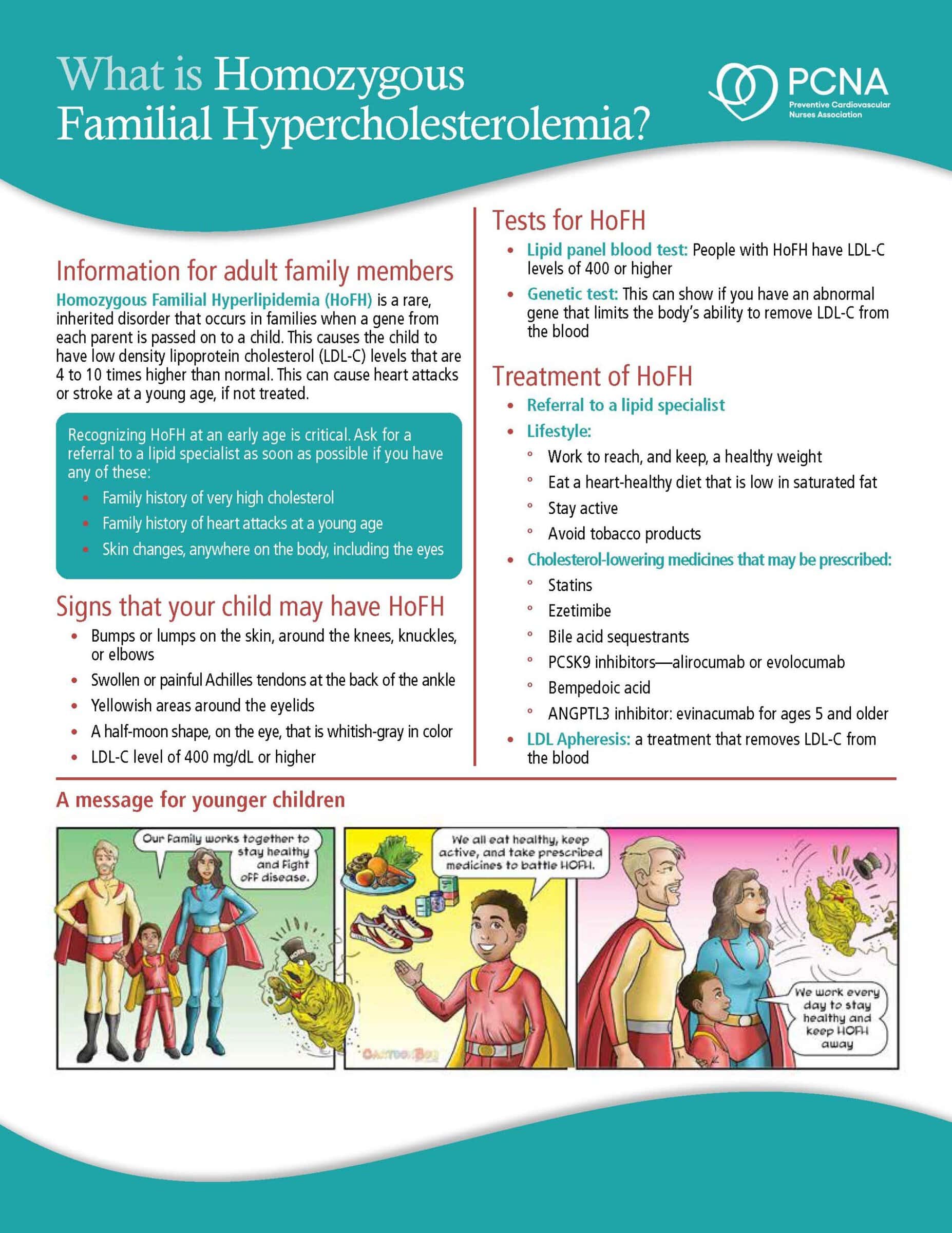
- What is Homozygous Familial Hypercholesterolemia fact sheet for families
I’m Yvonne Commodore-Mensah, Board President for PCNA. I’d like to welcome you to Heart to Heart Nurses. PCNA supports your professional journey with accessible continuing education, practical patient resources and a vibrant community that understands the unique challenges and rewards of cardiovascular nursing. Together, we’re advancing the knowledge that defines excellence in cardiac care while celebrating the difference you make every day.
Geralyn Warfield (host): (00:20)
I’d like to welcome our audience today to our conversation with Seth Martin where we’re going to be talking about genetic testing as it relates to lipid disorders. Could you introduce yourself to our audience, please?
Seth Martin (guest)
Absolutely great to be here. It’s an honor to be here at the PCNA conference here in Orlando. I am a cardiologist, specifically a preventive cardiologist at Johns Hopkins in Baltimore. And there I lead our lipid clinic.
So, lipids is a topic near and dear to my heart. have clinical centered around lipids, but I also do research in the field. And then I also lead our digital health lab. I have another interest in digital health and how that can play into team-based care and engaging patients in their care. So anyway, it’s great to be here. Looking forward to the conversation.
Geralyn Warfield (host): (01:09)
Well, thanks so much for taking time to speak with us today. As you mentioned in your introduction, you really have an interest in lipid management. But, specifically, that genetic component, that genetic testing component. Could you speak to that more for our audience?
Seth Martin (guest)
Absolutely. So, this is an area that is growing in the world of preventive cardiovascular care, and lipid management. Thanks in large part to one of our team members, a genetic counselor on our team, Emily Brown, we…About a decade ago, it was pretty uncommon to do genetic testing for lipid disorders. It was something that at our institution that we weren’t really doing.
And we were part of a national consortium of clinics that take care of patients with familial hypercholesterolemia. And really, it just wasn’t being done, outside of some focused research settings.
But the technology has improved over time. The cost has come down. And the evidence has built over the last decade.
And some of that has come from our center where we found that genetic testing can be quite helpful in making a definitive diagnosis of familial hypercholesterolemia. We found that it doubled the rate of being able to make a definitive diagnosis.
So that can be clarifying for the patient themselves. It also can be helpful for other reasons, including testing children or other family members.
So, as this information’s come about, now genetic testing has become quite a bit more common in patients specifically suspected to have familial hypercholesterolemia.
The National Lipid Association, and this was led by our very own Emily Brown, put out a statement about genetic testing in lipid disorders. And there was a class 1 recommendation, meaning the strongest recommendation, that this is something we should do for patients who are suspected of familial hypercholesterolemia.
There’s other genetic lipid disorders where there’s not as clear of a role of genetic testing, but specifically with familial hypercholesterolemia, there’s a clear role now. That’s really pretty new phenomenon. And we can talk more about FH. It’s very common and with major implications for cardiovascular disease.
Geralyn Warfield (host): (03:47)
I really appreciate the fact that you have kind of framed us in this previous decade because I think about what happened roughly 10 to 15 years ago when I was thinking about FH or lipid issues and those kinds of things—or even just overall—genetic testing was something that was kind of pie in the sky for a lot of us. It was too expensive. It wasn’t available in a lot of places.
And so having that information at your fingertips must make a big difference, particularly in these patients and their families with FH, doesn’t it?
Seth Martin (guest) (04:18)
Absolutely. It’s become something I offer to all those patients and their families. And many people say yes because we’re fortunate to have a genetic counselor that I can refer them to who can go through all the ins and outs of it before they do it—better than I could myself.
And the cost. I think what partly kind of tipped things over the edge for us was the cost was either going to be covered by insurance or if it wasn’t, the companies that were performing were saying we won’t charge anything more than $100 out of pocket. So, the capping, the amount that’s charged out of pocket. then that kind of cost strategy brought it within reason for many, many people. So yeah, it’s been quite helpful.
And it can be helpful for family planning or sometimes it’s helpful for treatment decisions. Or it’s even required in some cases for getting access to specialty medications.
One of the amazing stories of a patient that I’m going to share in my talk here [at the PCNA Cardiovascular Nursing Symposium] is Patricia, who’s given her permission to share her story.
Her story’s—actually, there’s an article about her on the Family Heart Foundation website. And she has homozygous FH inherited from both parents. And when we were looking to get her access to a new specialty medicine called evinacumab, it was actually required by her insurance that we showed the genetic testing results to get access to that medication.
So, in that case, it had treatment implications, but she also has two kids. And when you think about the family and confirming what’s going on with them. Once you identify the gene or the genes, you can then directly test for those in the children. And then it’s now information that is available to every future generation of the family.
Geralyn Warfield (host): (06:24)
So, are there any guidelines related to at what age this genetic testing could perhaps be used?
Seth Martin (guest): (06:30)
That’s a great question. So, I think when it comes to specifically genetic testing for lipid disorders, it’s probably this National Lipid Association statement that Emily Brown led that’s kind of the most detailed comprehensive resource in this area.
With respect to the age of diagnosing FH specifically, generally we want to start early.
So earlier is better. And generally, people are quite surprised to learn that this is something we want to diagnose and even start treating in children before the age of eight.
The more typical situation is you’re looking for heterozygous familial hypercholesterolemia, where you’re expecting that it’s been inherited from one parent but not both parents. So, although it’s important, it’s not as severe. In that type of case, generally, the information would be useful such that it would guide treatment initiation like a statin therapy at an early age.
Generally, it’s recommended to start that statin therapy by the age of eight in a child. But a family may want to get the information even earlier than that to know, to have the knowledge itself. But also, if it could affect kind of motivation around lifestyle, but hopefully lifestyle in a family that already has this genetic condition, they’d already be kind of tuned in to following the healthy diet and exercise.
Now, in someone in a family where both mom and dad are known to have heterozygous FH, or there’s family history of cardiovascular disease, there’s some suspicion of homozygous FH. That’d be where you’d want to even know earlier, typically by the age of two is the general recommendation.
So, my main message I want to get across is early. In childhood, as early as maybe two, but certainly before the age of eight, if familial hypercholesterolemia is suspected.
And this can be done through genetic testing, but it can be a reasonable strategy if blood is being taken to test the blood cholesterol levels as well.
But if a case of familial hypercholesterolemia is a little more borderline, and especially in a kid where the levels will tend to be lower, that’s where the genetic testing could be very clarifying because it may be kind of unclear whether they inherited the gene or not if the levels are borderline.
Geralyn Warfield (host): (09:25)
It sounds like it’s a great strategy to use at any age if there are triggers, if you will, that warrant this. If the cholesterol levels are abundantly high, much more than you’d see in this age group or that would be at healthy levels. If you’re seeing xanthomas or things like that, that might trigger you to think about something or as you’ve just described, if there’s family history, if one of the other family members has been tested, that’s important as well.
And I also hope you could speak to just a little bit more to what the role of that genetic counselor is. At what point or points are they involved in this conversation? So, you as a provider, for example, might say, ‘I think it might be time to do a genetic test.’ Do you then pass the patient off, if you will, to the genetic counselor? And what’s their role then?
Seth Martin (guest): (10:13)
Yeah, absolutely. Emily Brown is our genetic counselor, as I mentioned. She plays a critical role.
Generally, it is me passing it off. Usually, I’m seeing someone in clinic. I have that this is one of the next steps that we discuss. And if the patient is interested, I will then refer them to Emily.
And there’s sometimes patients that’ll make their way to her because they’re kind of identified through other channels. Sometimes patients are seeing another genetic counselor for another reason, and then they identify a concern for lipids and they get referred to Emily that way.
But we’re always working as a team. So, if she finds someone, she’ll ask me to see them. If I find someone, asking her to see them. Sometimes we’ll even, the visits will get coordinated on the same day, but most of the time they’re on different days.
I’ll be referring a patient to her, she’ll see them, we’ll get results not that long thereafter (maybe a few weeks later), and then I’ll have those results the next time I’m seeing the patient in clinic.
It’s very helpful, and she has the dedicated training in how to guide patients on the decision, both before and interpreting the results after.
So, she’s really critical. That’s why I became comfortable ordering genetic testing, because she took that kind of ownership and but she also knows how to coordinate the tests with the insurance with the testing companies, but also the insurance component of that. So all this kind of specialty knowledge that as a cardiologist it would be hard to kind of layer that on top of everything else that I’m already doing. So it really works well as a team effort.
Geralyn Warfield (host): (12:01)
We’re going to take a quick break, and we will be right back.
Geralyn Warfield (host):
Welcome back to our audience and we’re having a discussion about FH and genetics and I would like to pivot just a little bit. For those of us in our audience that don’t know too much about familial hypercholesterolemia, which is a mouthful, which is why I often will shorten it to FH. But let’s talk about what the prevalence is. How often might I see this in my clinical practice?
Seth Martin (guest): (12:25)
So, the answer is about 1 in 250 people in the US. There’s over a million people estimated in our country that have FH. It used to be thought to be 1 in 500. Now the current estimates are 1 in 250. So, it’s a lot of people out there.
So, if you look, you’ll find it. That’s why we all need to be very much vigilant looking for it, making the diagnosis.
And then when you make a diagnosis, t’s one person, but then it’s their family. So that it can have that cascading effect of finding more people with FH. So, it’s quite common.
And the ways to make the diagnosis, there’s clinical criteria. Some of them go by what we call the Dutch criteria. There’s also American Heart Association has criteria. There’s also some outside the US like the Simon Broom criteria.
Generally, what these criteria use are your LDL level. So, if it’s quite high, a classic severely elevated LDL is considered to be 190 mg/dL or more to be severely elevated. Although that should trigger the consideration of FH, you don’t have to be that high to have FH if you have a less severe gene mutation, if you’re younger and healthier and there’s reasons you could be below that level.
But a high LDL level plus a family history of high LDLs, but also early heart disease: women with heart disease before the age of 65, men before the age of 55, that plus the high LDL should trigger us to think FH.
But if you have the fortune of examining someone in the office, like I often do looking for these lightish rings around the eyes called corneal arcus or arcus senilis, especially if that’s before the age of 45, that’s pathognomonic for FH.
And then the xanthomas, as you mentioned earlier. They can show up as bumps in the hands, thickened Achilles tendons, even the Achilles tendons in more severe cases could be bulging out, so you kind of lose that inward curvature of the Achilles tendons. So, these are ways that we can diagnose FH.
But still we’re using our clinical judgment, the scoring system. It’s then the genetic testing that can really give that confirmation when you find the gene.
Now, I want to be clear, if we do genetic testing and it’s negative, that does not perfectly rule out FH. It’s possible that our current technology can’t detect the specific genetic pathogenic mutation that someone has. So, I want to be clear about that. But when it is positive, it’s quite useful.
So, FH is quite common.
We have readily available ways of diagnosing it.
And the cardiovascular implications are very important.
So, because of the high cumulative exposure to LDL levels from an early age over the early decades, there’s the risk of developing, then, early heart disease, advanced coronary artery disease, or other atherosclerotic cardiovascular disease.
So that’s the reason that clinical guidelines recommend early initiation of lipid-lowering therapy. And we’re now fortunate, we can get more into the landscape of lipid-lowering therapies. We’re very fortunate to have such highly effective non-statin therapies in addition to the statin therapy.
And a lot of the pioneering work here is thanks to patients with FH. PCSK9 inhibitors, the PCSK9 enzyme, the attention to that came from a French family that has a PCSK9 mutation that gives an FH phenotype.
And many of the clinical trials that have tested, been kind of the early trials testing drugs that ultimately made their way into clinical practice now, were first tested in patients with familial hypercholesterolemia.
So, this patient population has really led the way in helping us develop new therapies that then end up helping many, many people as well that don’t have FH.
Geralyn Warfield (host): (16:46)
So, I think one of the final things that you’d like to discuss with us is the shared decision-making and the team-based role when it comes to effective treatment of FH.
Seth Martin (guest): (16:55)
Absolutely. So, I’m very lucky to work with an amazing cardiovascular team that allows me to deliver the lipid care that we do.
I mentioned Emily Brown, our genetic counselor, but it’s also our nursing team, our pharmacy team, our office coordinators. So really that’s what makes it happen.
But the patient is at the center. It starts with that conversation in clinic about what’s going on, what the next options are. Now that we have such a number of lipid treatment options, I think it’s even more so the shared decision in anything is not just about statins and the type of statin, the intensity of statin, but also which of these other non-statin options is the best fit for you.
And so I really enjoy that conversation with patients, putting them at the center in their driver’s seat. there’s starting with that buy-in into the therapy, understanding that therapy and moving forward.
But our nursing team plays a big role. We have, first of all, an NP in our clinic who has more than a decade of lipid experience. And so she’s critical at providing a lot of the care to our patients with FH and other lipid disorders. And that’s Kathy Byrne who probably many people at PCNA will know.
And then Kiara is our nurse that works on our team. And she’s really critical at helping to follow up on some of our specialty medications that require prior authorization. Some of our PCSK9 inhibitor prior authorizations are in collaboration with our pharmacy, our specialty pharmacy, and we have a great team effort there.
Then a couple of them, really Kiara, takes the ownership of, in terms of the advanced lipid therapies. And I’m talking about the PCSK9 category, everything from evolocumab, alirocumab, inclisiran.
But then there’s also even more specialty, kind of less commonly used, like evinacumab. And so, Kiara plays a really key role in helping our patients access these critical therapies.
And then occasionally our lipid patients go for LDL apheresis. And Kathy Byrne has been an expert in that area for a long time and has been really tremendous at facilitating that.
So, it’s very much a team effort. We can come up with the best plans as the physician and patient in clinic, but unless we have the right team to support it being implemented well, it’s not going to work. So, I’m very lucky to work with a great cardiovascular team.
Geralyn Warfield (host): (19:33)
We’ve covered a lot of ground today. Do you have one final takeaway that you’d like to leave with our audience?
Seth Martin (guest): (19:38)
We have a lot of patients at cardiovascular risk out there and FH is one that should be prioritized given the severity of the LDL levels and early onset of heart disease. So, we should look for FH based on LDL levels, family history, genetic testing is playing an increasing role. And we now have a really rich armamentarium of treatments that can bring patients’ levels with FH, even if they’re starting very high, down to nice, low, optimal levels.
Geralyn Warfield (host): (20:15)
Fantastic. Thank you so much Seth Martin for spending time with us today. We’re really grateful to you.
Seth Martin (guest): (20:19)
Thank you.
Geralyn Warfield (host):
This is Geralyn Warfield, your host, and we will see you next time.
Thank you for joining us for this episode of Heart to Heart Nurses. We invite you to visit pcna.net for education and resources that will empower you to provide preventive cardiovascular care with confidence and expertise.
Topics
- Diagnostics and Devices
- Lipid Management
Published on
May 19, 2026
Listen on:
MD, MHS
Related Resources
Patient Education Handouts
What is Homozygous Familial Hypercholesterolemia? Fact Sheet
May 11, 2026