It is an exciting time in cardiovascular prevention and management, where we can work together to make a significant difference for our patients. New pharmacotherapies are changing the disease burden and improving our patients’ outcomes, regardless of circumstance. Guest Clyde Yancy, MD, MSc, MACC, MACP, FAH, FHFSA, FRCP, FASPC (Hon.), FPCNA (Hon.), provides data and inspiration for our actions every day.
Episode Resources
- SELECT Trial
- Health Equity Self-Assessment Tool: Take 10 minutes, identify your strengths, and get links to related resources.
Welcome to Heart to Heart Nurses, brought to you by the Preventive Cardiovascular Nurses Association. PCNA’s mission is to promote nurses as leaders in cardiovascular disease prevention and management.
Geralyn Warfield (host): I’d like to welcome our audience to today’s episode where we have the great pleasure of speaking with Clyde Yancy. I’m hoping you could introduce yourself to our audience.
Clyde Yancy (guest): I am so delighted to be here. This is the Preventive Cardiovascular Nursing Association meeting. What a humble privilege it is to be invited here.
My name is Claude Yancy. I’m a Professor of Medicine at Northwestern University Feinberg School of Medicine. And amongst my several obligations there, the one that brings me here is serving as Chief of Cardiology and additionally, I’m Vice Dean for Diversity Equity and Inclusion. Those of you who know me know I do a lot of other things, but those are really the two platforms that I bring to this meeting.
Geralyn Warfield (host): Well, we again are so grateful to you for taking time with [00:01:00] our audience today. One of the reasons that you’re here at the conference is I understand you’re receiving an honorary fellowship with PCNA. So, could you talk a little bit about your role within PCNA and nursing in general?
Clyde Yancy (guest): So, I must tell you, months ago, scrolling through emails, which as many of us receive, can be in the triple digit days sometimes. I come up on an email that has a very different heading, and it said, “honorary fellowship.’ Like, okay, what is this? And part of you in today’s world says, okay, is this straight or not? You open an email and your heart just, it speeds up. Your soul begins to smile because you realize that this incredibly important constituency, the people that really make healthcare happen, are looking at you and say, “We see semblances of our profession in you, and the way you comport yourself, in the way you care for patients.” [00:02:00]
None of us, none of us search for titles. None of us position ourselves to get more accolades. But when it does happen, and it comes from not only a trusted group, but a group whose ethos is about service and humility, that’s a pause moment. And so, it doesn’t matter what it is, just the fact that people that I revere, and respect so much have said, “We see something in you that reminds us of us, and we’d like to make that acknowledgement.”
It gives me yet another moment, though. I’ve been in medicine a few decades. A few decades, that’s correct. But I realize that everything I’ve learned, particularly at the bedside, was not taught to me by an attending physician or a resident, or a peer intern or any other such scenario. It was always the gentleness—sometimes the firmness—of a nurse.
A steady hand. A whispered voice. A careful [00:03:00] admonition. To help you do the right thing for the right patient at the right time. Nurses knew about quality long before doctors discovered. Nurses knew about safety long before doctors even phonated the word.
And so, I hold with deep reverence the profess of nursing. Because I know that’s the reason why many people are alive today—much more than what physicians do. I write orders and walk out of the room. Nurses take care of the patients. I couldn’t be more humble in their presence and more grateful for what they do.
So, this acknowledgement is great. Flying to Florida, I thought, “Wow. In 24 hours, I’m going to be a nurse.” How about that?
Geralyn Warfield (host): That’s awesome. Well, we again, really appreciate your partnership with nurses and other healthcare professionals with whom you deal every day. And it’s really that team-based care that really makes a difference for our patients.
And one of the things that you and I were speaking about right before we came on air [00:04:00] was how exciting it is to be in the field of cardiovascular care and cardiovascular management. And I’m hoping you could help share some of your enthusiasm about that as well.
Clyde Yancy (guest): So, you just said three very important words. Think about what you said. You said ‘team,’ you said ‘excitement,’ and you said ‘enthusiasm.’
Imagine some discipline in medicine where you can bring team, excitement, and enthusiasm into the same narrative. Unless it’s birthing babies. I don’t know what it is. But it is cardiovascular medicine now because cardiovascular science has given us so much substance, so much information, so many new guidelines.
We have data. We have evidence. And it’s remarkable to know that we’re changing, changing the natural history of disease.
It’s a privilege to be alive long enough and see where medicine was and where it is now. And it’s all because of scientific discovery, but also because of [00:05:00] implementation. So, it is fundamentally exciting. And you can hear the passion and the enthusiasm because I can look at a patient today and say, “I can do something about this. I literally can change this outcome.”
On the trip here, just last evening, I’m on the phone with a patient. “We can take care of this. We have strategies. What you read is correct, but it’s not contemporary. We can change this.”
My particular lens is heart failure. Oh, my goodness, we can do so much more in heart failure now than before—but it takes the team. And that’s why being here and working with the nurses, and I love that phraseology of the partnership that we all meld, not just me, but physicians across the country. Not just nurses, but physical therapists, respiratory therapists, particularly social workers, nutrition experts. It takes a team. And boy, it took us a long time to finally get here, but we here and we know that disease management is a team sport and patients are the better for it. [00:06:00]
Geralyn Warfield (host): We have had such an inspirational part of our conversation already, but we’re going to take just a brief break and we will be right back.
Geralyn Warfield (host): We’re back with Dr. Clyde Yancy, talking about the excitement, and the team-based care, and the importance of what we do each day as cardiovascular professionals.
And I know that there were some things that we talked about when it came to ways that we can actually impact our patients when it comes to disease states now that we weren’t able to do. You alluded to this right before we took our little break., I’m hoping you can talk a little bit more about the specifics of what we’re able to offer now that not very many years ago were not on the table.
Clyde Yancy (guest): So indeed, let’s explain why there’s enthusiasm. And let’s take three specific examples. For the first time, we’re actually able to look at persons who have a body mass index greater than 27.5 and declare that that is a condition. That’s not a slight, it’s not a [00:07:00] pejorative comment that is medical obesity and it has consequences. And we can declare that it’s a medical condition because we can intervene.
Yes, lifestyle will always be incredibly important. Diet and exercise or key in any conversation. But now that we have medical therapies originally targeted towards lowering blood sugar, but now with remarkable consequences that are favorable reducing body weight. But in addition to that, in addition to that, changing biology.
By changing the biology, we’re changing the burden of disease.
Just in November of 2023, several months before you and I are speaking today, we received extraordinary data from 17,000 patients, 42 countries in the world, patients already, already with preexisting cardiovascular disease, receiving once-weekly semaglutide therapy. A 20% reduction in the likelihood of subsequent [00:08:00] cardiac events.
The majority of the embedded cardiovascular disease was previous stroke, previous heart attack, 40% had heart failure, the majority had hypertension. These are real folk. These are the patients we see and treat every day. And now we know that if their body mass index is greater than 27.5 and we deploy semaglutide on a weekly basis, expecting about a 10% weight reduction, we see a change in the natural history. And it’s not just weight reduction because the changes happened before the weight reduction occurs.
It really does infer, and I’m using that word carefully, it really does infer, it doesn’t prove, but it infers that it’s a fundamental change in biology that is either cardioprotective or cardio restorative, but it makes a difference in cardiovascular outcomes.
And the data from what’s known as the SELECT trial was so profound that we saw the shortest all time ever for the FDA to grant a new indication for [00:09:00] a glucose-lowering drug because of these cardiovascular benefits. That’s pretty remarkable. So that’s the first reason why there is some excitement and enthusiasm.
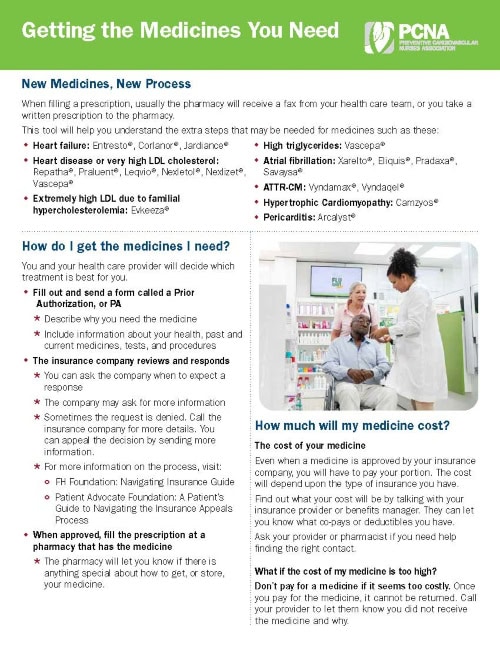
To be fair, there is a significant cost for these agents. Underwriters, insurers, even corporate entities, are bracing themselves for the cost implications. We have to work as a community to manage the cost, to understand the right patient, the right time, the right way, but nevertheless, the science is there and we can’t ignore it, and we have to address this and address it in a forthright manner.
The second thing: there is not a nurse in the prevention space like this meeting, or cardiologist who does preventive cardiology, and I do impart some of that as well, who hasn’t wrestled, and I’m using that word deliberately, with the tension about going on a statin therapy. Statins have changed our society. They fundamentally changed our society. But not everyone is comfortable taking a statin. The side effect profile is really quite modest, but there are some [00:10:00] real side effects—muscle aches in about 5 or 8%, a tendency towards hyperglycemia in about 7%. There are other reputed side effects, but none that have been validated in science, but that’s a tangent.
Accepting the fact that patients have the volition to say, “I will or won’t take this drug. I am concerned about those side effects.” That’s a fair conversation. But what makes the conversation work is just within the last 18 months, there’s so many more available agents that will lower blood cholesterol and facilitate care.
Think about a drug known as inclisiran, a silencing RNA compound, twice a year. Twice a year. And lowers LDL. Think about a drug like bempedoic acid. Totally non-statin related mechanisms of action. Lowers cholesterol. We’ve had ezetimibe for a really long time. Also beneficial. So, you think about this now, that we almost have a dropdown menu when someone comes [00:11:00] in and we have to manage their dyslipidemia.That’s for the good. And it gives us more tools. And whenever we have more tools, we can do a better job.
But there’s a third piece that is very exciting. We saw this gradual introduction of calcium assessment and calcium scoring in cardiovascular medicine. Some were very dismissive. Lots of us were wrestling with what do you do with the information if the calcium score is positive? Do you go straight to angiography? Do you do a stress test? What do we do with this? We know a lot more now. The most recent data helps inform what we should do. We know that normal is zero, but that doesn’t mean you’ll never get atherosclerosis. It means that at that moment in time there’s no calcium.
We know that a score, an Agatston score, between 1 and 125 is mild. Intensive lifestyle modification is a key consideration. A conversation about lipid-lowering therapy is quite appropriate.
125 to 300 to 400 there probably is established [00:12:00] disease. Not necessarily life-threatening or life-compelling, but it does require a bit more focus. And if there’s any symptom, follow it up with a stress test, but really intentional lifestyle modification and intentional lipid-lowering therapy along the lines of what we already talked about.
And boy, if it’s over 400 and certainly gets out to 800, that’s a really important conversation moment. There’s a shared decision-making time where we go through the risk and the benefits and we decide what would you want to have done at this point? Because we have a fairly high pretest likelihood that you have some coronary disease. We didn’t always have that opportunity, and now we have that.
So, in the last several minutes, think about what I’ve shared with you. We can treat medical obesity. We have more options than statin therapy to lower the lipid profile and attenuate for primary prevention, the risk of events, or prevent second events for secondary prevention.
And now we have maybe the best screening tool we’ve yet had. And for many people, the cost [00:13:00] of a calcium score is really quite an applicable.
Geralyn Warfield (host): The last thing I’d like us to spend a little time on is something that is the underpinning for everything else that we’re doing, and that is health equity. That we have remarkable opportunity to diagnose, to treat patients, but not necessarily is that happening equitably. I’m wondering if you could—I know we could spend years on this discussion—but just in our final moments together, provide some perspective on that particular topic for us.
Clyde Yancy (guest): So, health equity is part of my own academic scholarship, and I spend an extraordinary time studying it, writing about it, speaking about it, teaching others about it.
But let’s just be fundamentally clear. One thing we’ve learned over just recent years is that the absence of health in any one of us affects the health of all of us. That is a fait de complete. That’s a statement of fact.
With that awareness, then we have another reason for a certain kind of [00:14:00] comeuppance. Nearly 60% or greater of all health outcomes are not driven by biology. They’re driven by a person’s social circumstances.
Here’s the third comeuppance. If we use a broad lens, which we should, we’re not talking about race. We’re not talking about ethnicity. We’re talking about sex and gender. We’re talking about LGBTQI. We’re talking about older persons. We’re talking about people that live in rural America, about 50% of this country. We’re talking about people that have challenges with ambulation. We’re talking about people where language is different, English is not their first language.
When you consider the whole portfolio of people who come into the healthcare system from different backgrounds with different cultures, it’s important for us to understand that equity doesn’t mean equal.
Equal means doing the same thing for each person. But if people are coming to you [00:15:00] from different backgrounds, different perspectives, with either different enabling features or different disabling features, health and healthcare needs to accommodate that. Make an adjustment for it.
Because remember how this conversation started. The absence of health in any one of us affects the health of all of us. We are each other’s keeper, and we have to keep that in mind. All of these great things, all of that passion you heard me just talk about, the tenor of my voice has changed. It’s much more serious now.
Because we run the risk of having a greater divide across the board. Poor people, rural people, people with disabilities. Is that who we are? Is that our ethos? I think in nursing and medicine, that’s not our ethos. In medicine, we take an oath. And the oath says we will treat the patient in front of us regardless of circumstance.
So, health equity is deep. It is in the DNA of being a healthcare professional.
Geralyn Warfield (host): Dr. [00:16:00] Yancy, it has been such an incredible journey with you just in our short conversation today. And you have given us our marching orders in terms of what we need to do next.
And we are entirely grateful to you for all you do each and every day, just like every member of our audience, in making the world a better place for one another.
Clyde Yancy (guest): Thank you.
Geralyn Warfield (host): With that, this is Geralyn Warfield, your host, and we will see you next time.
Thank you for listening to Heart to Heart Nurses. We invite you to visit pcna.net for clinical resources, continuing education, and much more.
Topics
- Health Equity
- Obesity Management
- Risk Assessment and Management
Published on
June 18, 2024
Listen on:
MD, MSc, MACC, MACP, FAH, FHFSA, FRCP, FASPC (Hon.), FPCNA (Hon.)
Related Resources