






The intersection of risk factors for diabetes, obesity, hyperlipidemia, the liver, and the cardiovascular system is becoming increasingly evident, and so is the mult-system impacts of lifestyle and specific pharmacotherapies for prevention and treatment. Episode guests Joseph Saseen, PharmD, MNLA, FACC, CLS, and Emily Bankhead, MSN, FNP-BC, describe the positive impacts of healthcare professionals working collaboratively, and to the top of their scope of licensure, to effectively address multi-system disorders.
Episode Resources
- 2026 Multi-Society CKM Guideline
- PCNA CE Course: Cardiometabolic Treatments for Obesity
Thank you to Eli Lilly and Company for their independent support of this episode.
I’m Yvonne Commodore-Mensah, Board President for PCNA. I’d like to welcome you to Heart to Heart Nurses. PCNA supports your professional journey with accessible continuing education, practical patient resources and a vibrant community that understands the unique challenges and rewards of cardiovascular nursing. Together, we’re advancing the knowledge that defines excellence in cardiac care while celebrating the difference you make every day.
Geralyn Warfield (host): (00:32)
Welcome to today’s episode, the second in a 2-part series on cardiometabolic care. I’d like to welcome our guests, Joe Saseen and Emily Bankhead. I’d like them to introduce themselves to you. And Joe, we will start with you.
Joe Saseen (guest): (00:44)
Hello everyone, my name is Joe Saseen. I’m Associate Dean for Clinical Affairs and a Professor of Clinical Pharmacy at the University of Colorado Anschutz Medical Campus, Skaggs School of Pharmacy and Pharmaceutical Sciences. I work as a clinical pharmacist in cardiometabolic care and treat patients under collaborative protocols in our population.
Geralyn Warfield (host): (01:05)
Emily, could you introduce yourself to us, please?
Emily Bankhead (guest): (01:08)
My name is Emily Bankhead. I’m a Family Nurse Practitioner. I currently work at Pikes Peak ENT Allergy and Asthma, which is a private practice clinic in Colorado Springs. It’s a change of subject for me for most of my career. I’ve worked in cardiometabolic care, both as a registered nurse and a nurse practitioner. I’ve also worked with perinatal diabetes and in endocrinology. So that’s kind of my background.
Geralyn Warfield (host): (01:37)
Well, thank you so very much both of you for being here to share with us about this particular topic. And let’s go ahead and get started by starting the discussion around the complex interconnections that are encompassed by cardiometabolics. And maybe even what we’re calling cardiometabolics now and those types of things.
So, Joe, could you get us started with that part of the conversation?
Joe Saseen (guest): (01:59)
Sure, I like starting with history. I remember when I first started there was a thing called Syndrome X, which is this phenomenon where patients with insulin resistance or diabetes had a lot of other associated comorbidities like hypertension and heart disease.
And those terms have changed. I think most clinicians are very familiar with the term cardiometabolic or cardiometabolic disorders. And that that’s fine because it defines, sort of, a constellation of interconnected diseases where one causes the other, and perhaps the other one causes the other one in a vicious cycle. When really, it’s a constellation of interconnected organ systems and diseases that focus around a core abnormality such as insulin resistance.
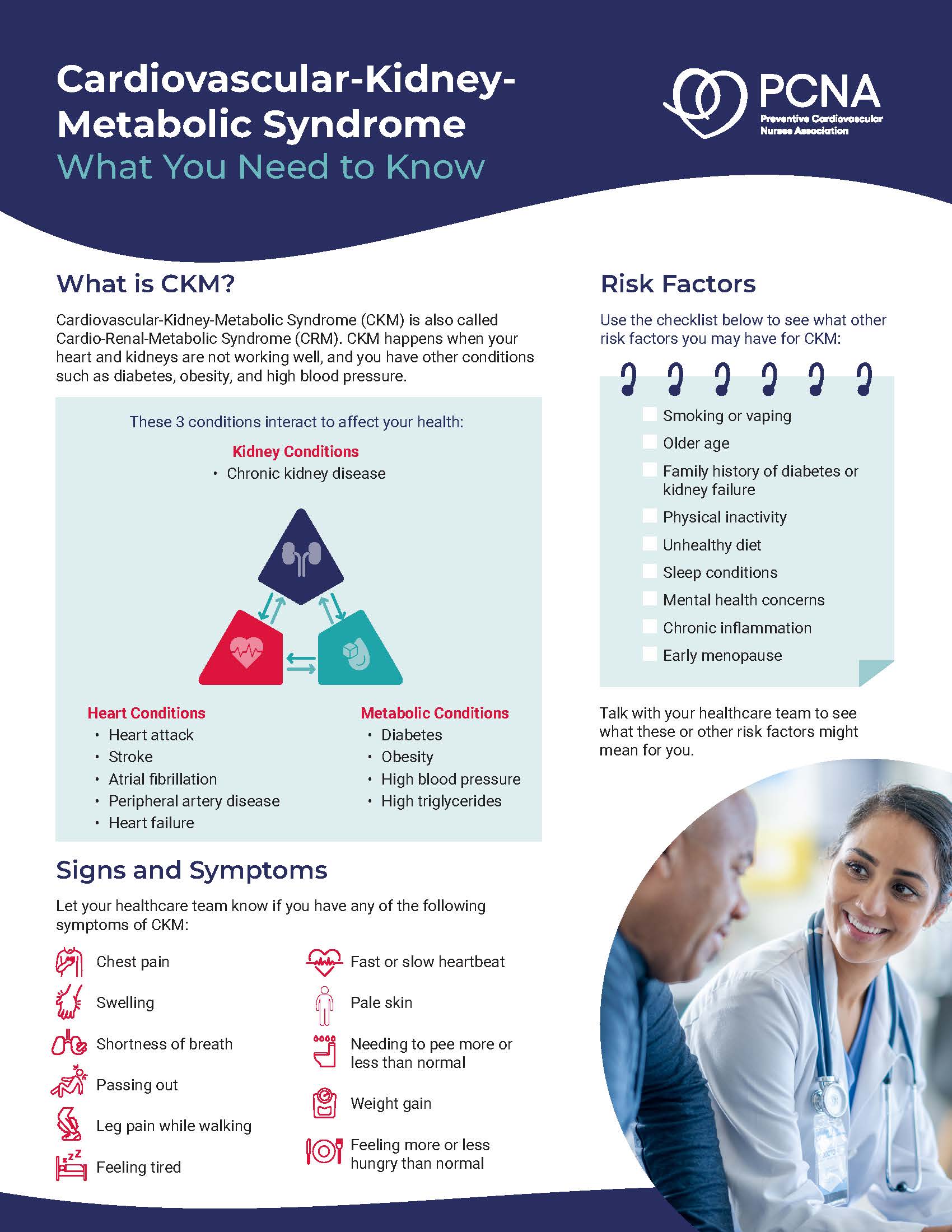
Some of the terminology has evolved. We now hear something called CKM syndrome, which is cardio, cardiac or cardiology (think of the heart there), kidney, the K, and M being metabolic. So, it’s a way of sort of not forgetting the kidney.
And just to be complete, I’ve even seen another one called Cardiac-L. I think it is, in the L stands for liver. So that’s a lot of organ systems.
But I think the population is very common. So, we have patients that have many of these interconnected disorders. And maybe the core feature or core risk factors are similar. Things like obesity, impaired glucose tolerance leading to insulin resistance or being caused by insulin resistance, really is at the core of the issue.
I think another thing that is common amongst cardiometabolic disorders is not just the long-term consequences, which are a multitude of morbidity and mortality related to mostly cardiovascular disease or cardiometabolic disease, when you add in the kidney and also the liver in there.
It’s not just the risk factors for it, which are similar, but also the drug therapies.
We’re at a point where you can add treatments for cardiometabolic diseases as a lot of them cross over that what helps one may help another one or multiple organ system diseases. So, when I think about cardiometabolics, I think of cardio kidney or CKM syndrome, which most people will call cardiometabolic diseases.
Emily Bankhead (guest): (04:27)
Following on that, I think that this evolution to include the whole system is kind of what we’ve been doing in the diabetes space for some time. When we were doing patient education for diabetes, there’s this concept of core defects, and we used to think that there were three, and we called them the terrible triumvirate. And then we had the ominous octet of eight core defects that involved the kidney and the liver and the brain and the gut. And then it became the egregious eleven.
And so, what I think is helpful in framing this is, it can seem really overwhelming. There’s all these body systems involved. But in teaching patients this is not just about your blood pressure, this is not just about your pancreas or your blood sugar, or diabetes; heart disease is a whole-body disease. But by doing three or four really simple, basic things, we can address a lot of these risks.
And so, it pulls into perspective that, number 1, that this is manageable, and number 2, that by making some small steps, you’re impacting a lot of different organs and a lot of different systems.
Joe Saseen (guest): (05:44)
Yeah, when I think about that, I also think of some of the basics that we know. Things start off with endothelial dysfunction and they evolve to different disease pathophysiologies. But an important thing that you made me think of is we shouldn’t stay stagnant because this field will continue to evolve and grow. Maybe there’ll be a new term for this. Maybe we’ll include gout or uric acid in there, or something else that is really important
And just remembering some of the basic things that started years ago related to lifestyle modification and modifying risk factors earlier in people’s lives really is important.
So, I think even though this can be a complicated disease pathophysiology and definition, condition, whatever we call it, I think some of the basics still are quite effective. We just continue to learn more and more and more.
And as I mentioned, the drugs do cross multiple organ systems and provide multiple benefits in patients with cardiometabolic, CKM syndrome. I think that’s going to continue also to evolve too and to the point where we even see access to these medicines maybe being easier with expanded FDA labels and indications. I’m hopeful, but I think we should keep an eye on that.
Geralyn Warfield (host): (07:05)
Well, you have aptly described how cardiometabolics affect so many body systems, so many different organs, and so many different healthcare professions, honestly, across the spectrum, from diabetes care through pharmacy, maybe you’re seeing cardiovascular individuals. I mean, there’s just so many individuals and so many different practices and so many different types of care that some of these patients are receiving.
What are some best practices or some strategies that we can offer that really help us hone in on effective team-based care to help improve outcomes for these patients that are dealing with so much?
Joe Saseen (guest): (07:45)
I think some of our best practices that we see traditionally published and proven come from the bigger academic medical systems or just big health systems. I don’t want to ignore smaller systems or more solo practices, so I will comment on that too.
But if we look into what’s defined as some of the best practices, they are integrated clinical care approaches which use multiple professionals. That use medical providers such as physicians and DOs, also APPs such as nurse practitioners and PAs. Clinical pharmacists, other nurses, other MAs. But I think the key is how they’re using them.
And the successful best practices really identify that each different individual healthcare professional brings something unique to the table. And really allowing them to what we call work at the top of their license.
So don’t just rely on the pharmacist to process prior authorizations, but allowing them to also modify drug therapy and intervene when appropriate within their scope. I can say that with nurses too, nurses don’t just support a function of a provider, they actually can educate patients and can work with devices and actually empower patients to actually care for themselves. So, I think the key is not just tapping into the unique skill set of our diverse provider population, but having a broader definition of who that is. It’s not just one type of professional. It’s more than one.
Finding a way to make that work is a best practice. And I think another part of best practice is making it sustainable. So we can talk in the ivory tower that everybody should have a physician and nurse, a this, that, and the other thing and a clinical pharmacist. But you have to find a way for it to be sustainable. So, we see the best practices, and this where it it’s more heavy in the bigger systems because they have more resources, is that they find a way to fund these people by billing for their services.
There’s a lot of states that allow billing for cognitive services by a clinical pharmacist, or by nurses that are not nurse practitioners, and MAs. And we really need to, I’ll use the word “exploit,” those opportunities and advocate for those opportunities because it allows high-functioning teams to support those team members.
I don’t want to ignore smaller health systems or solo practices because I often hear the feedback, “Oh, those solutions are great, but I don’t have all those resources available.” Well, unless you’re in a micro-practice where it’s only one person, you probably have at least one other healthcare professional and it might be your MA, it may be your nurse, it may be somebody else. Empower them. See what their skill set is and look to their scope and make sure that you’re pushing the boundary of that.
Emily Bankhead (guest): (10:30)
Joel, that was excellent. And I appreciate everything that you’ve had to say.
I want to second the importance of multidisciplinary care and encouraging every member of the team to hop in and contribute to the top of their scope of practice. As somebody who has not really worked in a big health system consistently, I’ve worked in the military, I’ve worked in private practice, I’ve seen cardiology clinic in a double-wide in a ranch town. I think it’s really important to be flexible and creative.
I think it can be easy to get overwhelmed of the scope of the disease. And I think sometimes just seeing what’s in front of you and working in your own little corner is a great place to start. I was in the military for several years in a nurse practitioner-run chronic disease clinic and we were able, because we had some flexibility and we made up a lot of stuff as we went, to eventually create a multidisciplinary continuing education course for primary care teams to come.
And we had great support from the leadership at the hospital I was at to teach primary care Mes and LPNs how to do foot exams and to talk about metabolic surgery. And it was something we did for two years. It was a lot of work, and it was really crazy, but that was something that in that situation really helped move the needle.
I’m in a situation now where I have a colleague who is retired from her diabetes career but is working in a local food bank. And she and another diabetes educator colleague started doing free diabetes classes in this food bank. And they had one class a year ago, and one of the patients came up to my colleague in the food bank when she was shopping and said, “I listened to everything that you’ve said, and I got my A1C down to 5.7%.”
And so, I think that working with where you are, whether that’s a large institution or a private practice or in a volunteer or school nurse capacity, wherever we are, there’s something to do. And it can seem very small and insignificant to start out, but continuing to push and to continuing to advocate for your patients is not only really exciting, but it’s very rewarding.
Geralyn Warfield (host): (12:58)
We’ve been talking about the interconnectedness of body systems and organ systems within individuals that have cardiometabolic syndrome, but also the interconnectedness of teams and individuals who are working from the healthcare professional standpoint to address the issues that these patients are facing. We’re going to take a quick break and we will be right back.
Geralyn Warfield (host)
We’re back on our discussion for cardiometabolic care.
And now that we have a better understanding of what cardiometabolics is and what effective care looks like, I’d like us to hone in a little bit more about CV nurses or cardiovascular nurses. How can we maximize adherence and outcomes in our roles as cardiovascular nurses?
Emily Bankhead (guest): (13:36)
As a nurse, I think we have so many opportunities to educate our patients and to listen to our patients that maybe we interact in a different way or a different approach than some of our other colleagues from other disciplines. I think listening to patients, listening to their concerns.
Joe had a really good point in a prior conversation about don’t assume somebody’s taking their medication. Ask them why and how, in a very non-judgmental, supportive role. If patients feel that they’re being criticized or that they’re failing, they’re less likely to be forthcoming with us.
And so, I think meeting patients where they are, celebrating their small victories and encouraging them, whether that’s they got out and walked for 10 minutes after a meal or they went from taking their cholesterol medicine 3 times a week to 5 times a week, that is still a win. And encouraging them in a hopeful way rather than a way of shaming or blaming, I think makes a big difference with patients’ motivation and adherence.
Joe Saseen (guest): (14:43)
I love that concept of celebrating all victories. Small victories, big victories, anything, because I think it really comes towards motivational interviewing, what works for your patient.
And I think the more that you can show to your patient—and nurses do a really good job of this, at least the ones that I’ve worked with—of not only being relatable to their patients, but showing genuine care for them as people, and aligning their successes with what their goals are, it’s very important. So, I think that that is not the only, but one secret to success for maximizing inheritance and outcomes.
Geralyn Warfield (host): (15:21)
I have one final question for each of you, and that is what one key takeaway would you like to leave with our audience about our conversation today? Joe, why don’t we start with you?
Joe Saseen (guest): (15:30)
I’d say be open to innovation. Not a lot of people want to hear with what’s around the corner as far as things like, dare I say AI, but I will say AI. I have a love-hate relationship with AI, but I think it’s not going away. And I think we need to find ways to leverage newer ways of doing traditional treatments.
Because our traditional treatments are our foundation, but we have to implement them in unique ways. And I often think of with prior authorizations, which are sort of the bane of my existence at times. But we’re going to get to a point where maybe AI helps us more than we think.
And maybe helps your patient as far as what’s done before a medical encounter, whether that’s face -to-face or telephonically, to tee up a patient, in a positive way, or in the way that we want them to go, or which is towards the truth. So, I think being open to innovation and trying to lean into when it helps
fill our needs is going to be our secret to success.
Emily Bankhead (guest): (16:35)
I appreciate what you said, I 100% agree with you.
I think it’s easy as healthcare workers to get overwhelmed or g to get discouraged, whether it’s with just all the work there is, or even if you have that one patient that is just really struggling and doesn’t seem to be understanding or adhering.
And I think taking a step back ,and never giving up, realizing that somebody might not be ready to change today—whether that’s a patient or an administrator or a health system—to not give up because the stakes are so high.
And we want to keep trying because people will, not everyone changes when and how we want them to, but it’s so important even to reach one or two people or make one or two small changes can really impact long-term outcomes for them.
Geralyn Warfield (host): (17:30)
We are so grateful to both of our guests today, Joe Saseenand Emily Bankhead. Thank you for sharing your expertise and insights with our audience.
I also want to remind our audience that this is the 2nd in a two-part episode series. And I would encourage you to listen or watch the other episode and also refer to the show notes for additional resources and information about this topic.
I’d also like to thank Eli Lilly and Company for their support of this mini-series.
And this is your host, Geralyn Warfield, and we will see you next time.
Thank you for joining us for this episode of Heart to Heart Nurses. We invite you to visit pcna.net for education and resources that will empower you to provide preventive cardiovascular care with confidence and expertise.
Topics
- Diabetes
- Kidney Disease
- Lipid Management
- Obesity Management
Published on
June 30, 2026
Listen on:

PharmD, FNLA, CLS

MSN, FNP-BC
Related Resources
Online Interactive Guides
Diabetes and Your Heart: Close Connections Online Interactive Patient Tool
June 12, 2025

Patient Education Handouts
Cardiovascular-Kidney-Metabolic Syndrome: What You Need to Know
May 11, 2026