Identifying and managing PAD requires a head-to-toe strategy. Guest Tiffany Staab, RN, FNP, MSN, describes the four PAD stages, how the disease disproportionately affects Black patients, and the importance of listening to patient symptoms and observing lower limbs to help stem the tide of PAD-related amputations.
Episode Resources
- PCNA PAD resources
- American Heart Association’s PAD heat map
Tiffany Staab podcast episode transcript
[00:00:00] I’m Erin Ferranti, board president for PCNA, and I’d like to welcome you to this episode of the Heart to Heart Nurses Podcast. PCNA is the proud home of cardiovascular nurses and one of the leading figures in the fight against cardiovascular disease. We have the resources you need for your day-to-day practice or to follow your passion to new areas of learning and growth.
Geralyn Warfield (host): (00:19)
Well, I’d like to welcome today’s audience to our conversation about PAD. And for our discussion today, I’m being joined by Tiffany Staab. Tiffany, could you introduce yourself to our audience?
Tiffany Staab (guest): (00:29)
My name is Tiffany Staab I’m a nurse practitioner. I work in general cardiology and general vascular cardiology. So, I don’t do the procedural aspect of things, but I do the preventative management or the post-procedural management of these patients. And I work at Mayo Clinic in Arizona.
Geralyn Warfield (host): (00:46)
Well, Tiffany, thank you so very much for being here. For our audience, maybe that’s not quite as familiar with PAD, could you describe what it is?
Tiffany Staab (guest): (00:53)
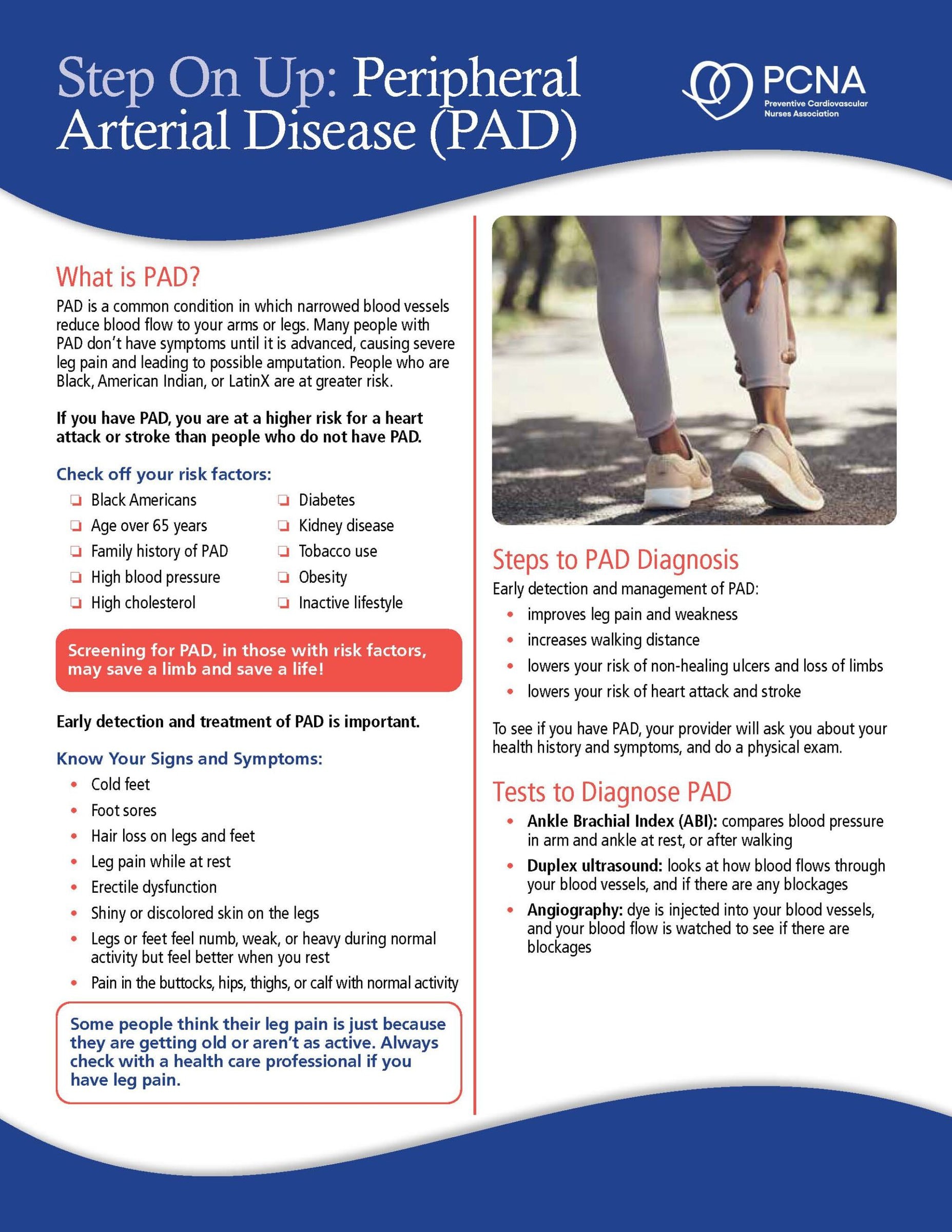
So, it is lack of blood flow to the lower extremities. And a few things I’d like to point out is when I was at ACC last week actually, so Dr. Jeffrey Allen said something very powerful that really resonated with me was peripheral arterial disease is the disease, it’s an epidemic of malpractice or medical neglect. And wow! The big thing, it’s interesting when you talk to your colleagues. I’m like, “Do you look at their feet? Do you look at their legs?”
Half of them say no. Half of them don’t want to look at the legs, the feet. But you do need to look at the legs. You do need to look at these feet.
And there are four substrates with peripheral arterial disease. And they can flow from one to the other. And they can get revascularized. And they can get improvement. And then they can go back to being worse.
So, first is asymptomatic peripheral arterial disease. That’s mostly about 20-59% of the population. Those individuals have some atherosclerotic disease in the lower extremities, but may not have a lot of symptoms with it. So, they may not be even aware of it.
Then you go into chronic symptomatic peripheral arterial disease. And those are individuals who do have classic claudication symptoms. So, they have pain with walking, they may have numbness, tingling, or even what I hear most of the time, which people don’t talk about is they feel like they hit a wall when they’re walking. So, they’ve like, “I used to be able to walk two miles. Now I’m like walking one mile and I feel like my legs can’t go on any more.”
And I’m like, “Well, is it painful? Does it hurt?”
“No, not so much.”
That’s a red flag. It is. About 30% of the population have the typical symptoms, which is pain with walking, cramping, numbness and tingling, discoloration in the feet. So that’s not a lot of the population, actually. It’s a lot of unsure, what am I feeling? Is this what I’m feeling?
Then you have your acute limb ischemia, which is critical. These patients are severe, less than two weeks of severe symptoms, paleness, no pulses. They need to be vascularized quickly. They need to be in the hospital.
Then unfortunately, you do have your chronic limb-threatening ischemia, which is similar to acute limb ischemia, but now it’s gone on for greater than two weeks. “Oh, I have this ulceration,” or “I have…my toe looks off. What is that? Why is that? Why do I hurt so much?” These individuals have a high mortality rate, actually. About 30% in like the first five years. It’s pretty significant.
And I feel like peripheral arterial disease is like the forgotten love child of atherosclerotic disease. We just worry about the carotids, we worry about the heart, and then the legs are like the last thing for us to think about.
But, quality of life is very important for these patients. The problem is, you can have someone with asymptomatic, then they can become chronic symptomatic, then they can go straight to acute and then get revascularized. So, then they’re going back to maybe asymptomatic, then they can go back then to chronic. And it’s a never-ending cycle. It really is.
And once you get revascularized, or if you get bypass or endovascular repair, it’s not the end. A lot of people think it is. Like, “I’m done. I got fixed. I don’t have to worry about this again.” Unfortunately, no. The need for revascularization keeps on going.
Geralyn Warfield (host): (04:21)
Is there a particular segment of the population that this affects more than others?
Tiffany Staab (guest): (04:25)
So, fourfold in African Americans and Blacks. And what’s also surprising is Black women get diagnosed 10 years later than Black men.
Geralyn Warfield (host): (04:35)
Now do you suppose, or does the research pan out, that this is because they are avoiding reporting their symptoms or they don’t recognize them? Is there any one, or more than one, factor that affects that?
Tiffany Staab (guest): (04:48)
I think it’s all of that, honestly. I feel like, and I will say in my practice, women tend to be the caregivers of the family, and they don’t seek assistance. Or when they do, it’s already, they’ve got a wound on their toe, they’ve got a wound on their foot. “This has now been present for a week or two. Now I need to do something about it.”
I think it’s a large portion of that, but also access to care is very limited, especially in your rural areas. The American Heart Association does an excellent job of what they call heat maps, where you can show where there’s major adverse limb events, meaning amputation, and take a look at that map. Where are you at on that map? Arizona’s not too bad, but there are certain parts, you know, rural over urban. The access to care is also a large portion of it, too.
Geralyn Warfield (host): (05:40)
We will definitely put a link to that map in the show notes. So, if you’re interested in that, make sure you check out the show notes.
That is one of the most compelling things that I’ve heard about PAD recently is that it’s significant increase in limb amputations in particularly in Black and African-American populations. And what a travesty that is.
Tiffany Staab (guest):
That is.
Geralyn Warfield (host):
There’s no reason that it has to be that bad.
It’s incumbent on all of us, as you said, to basically kind of look below the heart. Make sure that we are looking at the person as a whole individual and from head to toe.
Tiffany Staab (guest):
Yes.
Geralyn Warfield (host):
And checking out what’s happening, right? So, I know that walking and claudication causes this real issue with walking. I’ve had family members that have had PAD and it’s just astounding to me how much PAD impacts their ability to walk. (06:33) And even just getting, doing a loop around the grocery store is sometimes impossible. So, they’re looking for that display of patio furniture halfway around the store because they just can’t walk anymore.
So, how does a walking program for somebody who can’t really walk, how does that work?
Tiffany Staab (guest):
It’s a good question. So, we have a few of them in Arizona, but not a lot. And they’re part of cardiac rehab.
It’s actually what we call the PAD walking program. And so, it is a supervised exercise walking on a treadmill for at least 30 to 45 minutes and then increasing incline. So, getting that circulation going, getting those muscles engaged.
And then, it hurts. And I don’t know how many times my patients say, “I just can’t do it.”
And I’m like, “I know you can’t, but you’ve got to do it. You’ve got to get up, you’ve got to go walking until that pain, until you feel it, and then try to push a little bit past that. Do little bit of increments every day and then you’ll find you’ll start going farther and farther and farther.”
I’m going to be honest with you, the access to a PAD walking program, even in my area in Arizona, is very limited. Mayo Clinic has one, HonorHealth has one, Banner has one, and then there’s only two other locations that have them.
And the other thing is access to it. People are working, or you can’t walk so you can’t get to the PAD walking program because you’re limited. Or you’re in a wheelchair and you need assistance.
And so, there is home supervised, but it’s not very well utilized. And I don’t feel that there’s actually a lot in my area of Arizona that I can offer my patients for this.
So, what I do tell them, I said, “Okay, if you can have someone at least take you to a couple sessions, learn what you’re doing there exercise-wise. Listen to the education. Of course, there’s going to be the diet aspect of things, the cholesterol, blood pressure, diabetes, no smoking. All of that all plays a factor like it does with everything else. But take that what you learn and then okay, implement that at home.”
But then again, quality of life becomes a discussion. And that is where okay, if we’ve tried at least 3-6 months of very supervised walking and we’re not getting any improvement in symptoms, then revascularization is something we could consider.
Geralyn Warfield (host): (08:53)
And what does revascularization typically entail?
Tiffany Staab (guest): (08:56)
So, that’s a good thing. So, you can either do a bypass procedure, or you can endovascularly stent, or angioplasty.
There is a new one on the horizon, at American College [of Cardiology], they briefly touched on it. I’m not going to kind of dive into it, but it’s called scaffolding, which has actually good, and that’s lower, below-the-knee intervention that’s showing some good promising. So, there’s going to be some things on the horizon, I think in the future.
But most of it is stenting, bypass, and femoral bypass, iliac bypass, things like that. But I’m going to be honest with you, again, it’s not one and done. And a lot of people think it’s one and done. And it’s not.
So, when they feel better, then that is a time we need to prioritize nursing staff, education. “All right, get walking now. You no longer have the symptoms. You no longer have those. Work on them now so you don’t have to be revascularized again later down the way.”
So, walking will be number one. But can everyone do it? No.
And I also think cilostazol is underutilized quite a bit actually in the PAD. However, there is a black box warning for heart failure and most of these patients have coronary artery disease, ischemic heart disease, HFpEF, so then you’re kind of limited on the use of that.
But it does show, because it’s both a vasodilator and antiplatelet medication combination, people tend to walk farther. I kind of save that for my patients who can’t undergo endovascular repair or bypass because there’s just no targets and they’re so severe. So, it’s kind of my last resort at this point in time.
Geralyn Warfield (host): (10:35)
So, there are some options for our patients with PAD. They might be few and far between and they might have to be repeated, is what I’ve learned from our conversation thus far.
Tiffany Staab (guest): (10:43)
Yes.
Geralyn Warfield (host): Okay, well we are going to take a quick break and we will be right back.
Geralyn Warfield (host): We are back with Tiffany Staab and we are talking about PAD and I know that you wanted to discuss a little bit more about disparities and prevention and how we best can help our patients to not have to get to the point where they need revascularization surgeries or things like that. So could you share with us about that?
Tiffany Staab (guest): (11:05)
Yes. So, those that are at the highest risk are current smokers and those who are diabetic. So, if you have a patient who just meets one of those criteria, take a look at their feet. If you’re a nurse and you’re rooming the patient, take a look at their feet. Take a look at their ankles. Take a look at their shins. Take a look at their legs. That is a good place to start.
The other thing is, I feel like there’s a call to action from American Heart Association to promote more education, not just to the patients, but to our healthcare individuals who provide that. And the nurses are going to be always first line, and you guys are going to be our best friends. So, if you see something, or if a patient just offhandedly says, “You know, I have a calf discomfort every once in a while, but I don’t think that’s anything,” it could be something. Keep your eyes open, keep your eyes pealed. Keep looking.
Geralyn Warfield (host): (12:04)
Sounds great. So, the onus is on us…
Tiffany Staab (guest):
It is.
Geralyn Warfield (host):
…to try and fair it out, information to try and sleuth and see what the causes are. That’s great.
All right, Tiffany, I have one final question for you and that is what key takeaway would you like our audience to leave with?
Tiffany Staab (guest): (12:18)
I think our nurses are underutilized with PAD. They are our first line. And they are our eyes, our ears, for both patients and ourselves. And they can be our first line to get in this. No more chronic limb-threatening ischemia. No more acute limb ischemia. I mean, come on. No more amputations. Let’s do this. It’s doable.
Geralyn Warfield (host): (12:41)
It’s doable if we all work together.
Tiffany Staab (guest):
Correct.
Geralyn Warfield (host):
Awesome. So, thank you so very much, Tiffany, for being here today and inspiring us to action. So, whenever you’re listening to this, I encourage you to look at your next patient’s feet, if it’s appropriate.
So, thanks so much for being with us. This is your host, Geralyn Warfield, and we will see you next time.
Thank you for listening to Heart to Heart Nurses. Visit PCNA.net for clinical resources, continuing education, and much more.
Topics
- PAD
Published on
September 16, 2025
Listen on:

FNP-MSN
Related Resources