")
Elevated LDL-C is directly associated with the development of ASCVD. Learn about current treatments, barriers in applying guideline-directed therapies, strategies for prioritizing LDL-C in clinical practice, combatting misinformation, and utilizing shared decision-making from guests Kim Prado, DNP, AGPCNP-BC, and Binu Koirala, PhD, MGS, RN, FAAN, FPCNA.
This episode is supported by Amgen, Inc.
Episode Resources
Geralyn Warfield (host): Welcome to today’s episode where we are going to be discussing the lowering of LDL-C and the importance of that in clinical practice. I’m joined by two experts in the field, Binu Koirala and Kimberly Prado, and I’m going to have them introduce themselves to you. Kim, could you start by introducing yourself?
Dr. Kimberly Prado (Guest): Absolutely, Geralyn. And thank you so much for having us here. I was very delighted, especially since I love your podcast. My name is Dr. Kimberly Prado. I am an Associate Professor at Rutgers University within the College of Nursing. I also practice in cardiology at Summit Health. And I am also a co-chair for the PCNA Northern Chapter of New Jersey.
Geralyn Warfield (host): Perfect, thank you so much. Binu, how about you?
Binu Koirala (Guest): Sure. Thank you so much for having me here, too. I’m really excited for the topic today. And my introduction: I’m Binu Koirala. I’m an Assistant Professor at the Johns Hopkins University School of Nursing.
My practice and research expertise include cardiovascular risk prevention and management. And I also serve as Maryland chapter leader and Project Development and Review Committee member at PCNA. Really excited to be here today.
Geralyn Warfield (host): Well, I’m very grateful to you both for spending time with us and our audience, sharing your expertise. And so, just to make sure we all have our information correct, Binu, I’m hoping you could talk just a little bit about the interrelationship of ASCVD and LDL-C.
Binu Koirala (Guest): Sounds good. And I think that’s a perfect start to talk about why LDL-C is important. So, I’ll just start with what is ASCVD. So, when we are referring to ASCVD, I’ll start with the data from American Heart Association. So, between 2017 and 2020, around 128 million American adults had some form of cardiovascular disease. And when we also look into data, there were more than 25% of the people who had higher LDL-C levels.
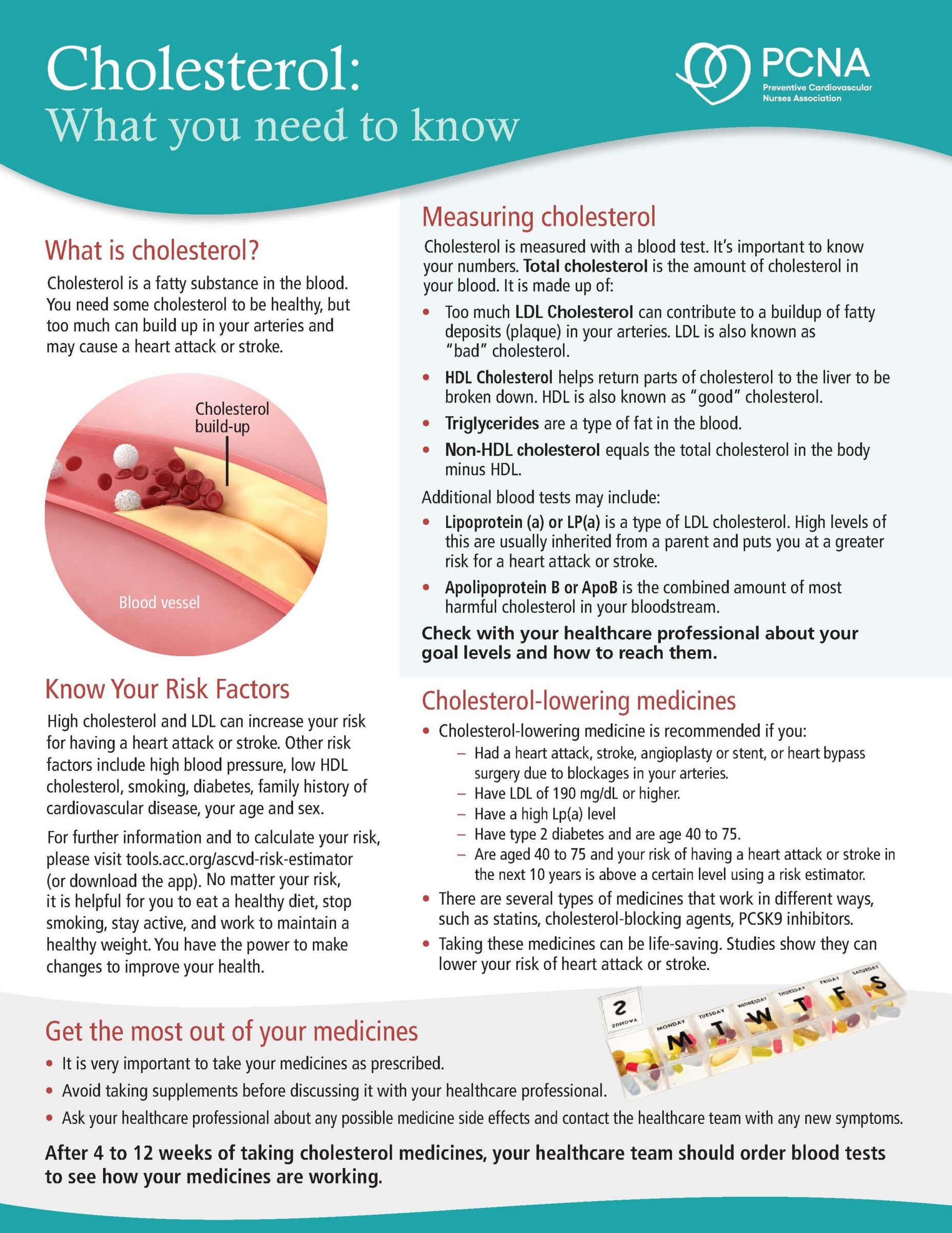
LDL-C is really important because elevated LDL-C level is well understood to be directly associated with the development of ASCVD, and which is caused by the plaque buildup in the arterial walls limiting the blood flow to the different organs. And which will cause different conditions such as coronary heart disease, cerebrovascular disease, peripheral arterial disease, and aortic atherosclerotic disease.
So, LDL-C is directly associated with ASCVD. So, it’s really important to control LDL-C levels to prevent the ASCVD episodes.
And, despite the advances in pharmacological treatment, higher cholesterol remains a significant problem in the US and globally, and we really need effective approaches to manage it.
Kim, would you like to add more?
Dr. Kimberly Prado (Guest): Oh, of course. Your statistics are very significant and reflect how coronary artery disease is still the leading cause of death of both men and women worldwide.
And we know that since 2015, heart disease deaths have continued to rise since then, and thought to have been caused, one of the thoughts, was caused due to the obesity epidemic. And yet with heart attacks and strokes and these life-changing events, this can lead to disability and possibly death—and certainly can be prevented.
We know from landmark trials, like the JUPITER trial, showed a significant reduction in major cardiovascular events, because of the thought of the LDL-lowering—which had a 50 % lowering in that particular trial with rosuvastatin. And also, in that trial showed it had the high sensitivity C-reactive marker, protein marker, was also lowered 37%.
The other landmark trial that comes to my mind is the ASTEROID trial. That trial was, I found, very significant because of the power of that pleiotropic effect that statins can provide. You know that pleiotropic effect is that plaque stabilization within the coronary artery. And it found also the whole targeting of that LDL to goal not only helped prevent plaque progression, but plaque regression.
Everybody was so excited when they realized we could get plaque regression from medication. So, because of the benefits of statin therapy, reducing cardiovascular events, there’s still, as we know, the guidelines show first-line therapy. However, you know, and that’s always in addition to, of course, your good lifestyle, diet and exercise.
However, sometimes individuals have a difficult time tolerating statins, and/or they didn’t get to goal with statin by itself, or they need combination therapy. And so sometimes we need to switch to different lipid-lowering agents or combine them.
Geralyn Warfield (host): That’s a great segue, Kim, into our next part of our episode, which is really talking about, beyond statins, what are some current medications that are available for us to use to help our patients lower their LDL-C?
Dr. Kimberly Prado (Guest): Well, we have some very good tools to utilize. There are so many great medications out there that, depending on how the patient presents, can make all the difference with that combination therapy.
So, let’s say, for example, a client comes in and we have them on statin therapy, and they either don’t tolerate max dose or you just don’t have their LDL to goal yet.
Well, ezetimibe is—Zetia® is the brand, ezetimibe is the generic—is a great extra choice to pick to add as combination therapy because that medication can inhibit the cholesterol absorption in the small intestine.
And that works beautifully because sometimes—and I don’t know if you’ve heard the term like with “gut absorbers”—clients, you start them on statin therapy, you’re expecting that nice significant LDL-reduction, and it just didn’t happen to what you want it. This way, sometimes, their individuals can have this increased compensatory cholesterol absorption within their own body within the gut. So, by adding ezetimibe, that helps block that absorption. And now, instead of getting only a 6% further reduction in your LDL; you’ll get a 20% further LDL reduction to that additional statin dose reduction. So really does a nice job getting those LDLs to goal.
Another option, which works beautifully, especially if individuals have difficulties tolerating statins—you know, we all have seen those individuals that have myalgias or have some type of adverse effects and they try multiple therapies of different statins and they still struggle.
In those cases, PCSK9 inhibitors, which is a monoclonal antibody, works beautifully. Repatha®, which is one of the PCSK9 inhibitors, have remarkably lowered LDL reduction up to 60%. And what I absolutely love in addition to that, it is also found to lower that Lp(a), the lipoprotein A by 20%, which is, you know, Lp(a) carries cholesterol in the blood. It’s pro-inflammatory, pro-thrombotic; it just adds to the risk of that individual. So that is also another nice choice.
The only con, downside I should say, individuals, it’s an injectable. Not everybody likes an injectable. They find a pill sometimes it’s a little easier to use. But thank goodness for technology. The pre-filled syringes with auto injectors sometimes make it not too, not as bad as what the client would anticipate.
The other part that sometimes is a struggle is coverage from insurance. But many times, if we get on the phone as providers and talk to the insurance companies, which I know takes time, a lot of times it can work out, especially if the individual had not tolerated other statin therapy.
So, these are a few off the top of my mind that focus in on the LDL. I mean, certainly there’s other therapies that focus in like omega fatty acids with Lovaza® and fenofibrates that focus in on the triglycerides, but for lowering LDL, those are really good items to have in your toolbox, so to speak.
Binu Koirala (Guest): Thank you, Kim, for the wonderful information. And I just want to reiterate three key messages here. So, based on the research and learning from our practice, the use of a statin to lower LDL remains the key for the prevention and management of ASCVD.
The second thing is some patients who are unwilling or unable to tolerate statin therapy, or while others who fail to lower the LDL levels despite the use of the statin, in those cases, we may consider non-statin therapy to LDL management. And we can be sure that non-statin therapies for LDL management have been shown to reduce cardiovascular risk when given as an adjunct or alternative to statin therapy.
So, it’s safe to use and has been approved to use per LDL-lowering agents. I just wanted to highlight those three key messages here.
Dr. Kimberly Prado (Guest): Good point.
Geralyn Warfield (host): Thank you so much for sharing that great information. We’re going to take a quick break and we will be right back.
Geralyn Warfield (host): We’re back with our discussion on LDL-C-lowering opportunities that we have in clinical practice, with Binu Koirala and Kim Prado. And I’d like us to shift just a little bit into another part of actual clinical practice, which we could probably spend hours discussing. But what do you see as some of the barriers for clinical practice in terms of applying guideline-directed therapies for these patients that have elevated LDL-C?
Binu Koirala (Guest): Very good question. And so, when we start this discussion, let’s start with the process. So, at first, I feel like some of the barriers are associated with appropriate risk screening. So, are we doing these risk screening on time or regularly? And if we are, are we re-evaluating those risks? And do our patients understand these risks and importance of a statin or non-statin therapies to lower LDL-C labels?
So, we really need to think about where we are and how we are prioritizing identifying the high-risk population.
And also, actually, I feel like this is the right time to disclose that in my family, my husband has familial hypercholesterolemia and my mom also have higher cholesterol. And whenever I think about barriers of these therapies, I think one big question that comes in my mind is when to start treatment versus when it should be started.
So let me explain here a little bit more. What I mean here is multiple studies have shown that it is not only the level of LDL-C which matters, but also the exposure to elevated LDL-C levels, which is the like LDL-C years or exposure to elevated cholesterol. These have direct relationship with the ASCVD risk.
And as a family member of someone who has higher cholesterol, I think my husband and my mom were struggling to start these therapies on time because of so many things, such as preference to lower cholesterol with lifestyle changes, rather than just starting the medication because it requires commitment, also trouble in remembering the taking medication, refill issues, sometimes it’s just the dislike about the medication in general and side effects.
So, I can see our patients who are thinking through these parts, and these could be the some of the barriers for using guideline-directed medical therapies for the management of LDL-C.
So, we need to communicate these issues or explore these issues with the patients and identify the goals together. And with this, another important part is making accurate documentation of all these things that we do or that I just mentioned. Risk assessment, patient preferences, treatment decisions and goals, an evaluation of these therapies that needs to be regular and properly documented for further follow-up and continuity of care.
Dr. Kimberly Prado (Guest): No, I agree with you, Binu. Well said. And barriers definitely involve also patients with their non-adherence to meds, their costs, the side effects, statin intolerance. There’s so many types of barriers and you covered it nicely.
There’s certainly what I’ve seen sometimes with individuals out there, a lack of understanding of the importance of therapy. And that’s where many times early diagnostic tests can show them if like coronary calcium scores if they feel they have misconceptions of what the therapy is, and the diagnostic tests can show them if they have plaque already.
But like you said, addressing the barriers with communication, patient education, even though sometimes that’s very challenging with all the time constraints that can sometimes occur during office visits, it is so key that communication is so important and patient education is so important and can make all the difference in that individual. And focusing and giving specialized care to that individual makes all the difference. I agree.
Geralyn Warfield (host): Kim, you have again created a great segue for our next part of our episode, which is really to talk about how we can take the time for this very important topic of LDL-C in these clinical visits, which are sometimes so tight when it comes to all the things that are trying to be accomplished in a very short amount of time.
What are some strategies that we could do to help clinicians, to help healthcare professionals who are working with patients to make this a priority?
Dr. Kimberly Prado (Guest): Great question. I mean, I think for me, the biggest importance is identifying those that are at risk early so that we can focus on prevention instead of reaction. So, utilizing those tools are so important. Coronary calcium scores, like I mentioned before, is absolutely perfect for those individuals at intermediate risk.
I mean, we all know how to treat individuals that have high risk, established coronary disease and those that have no risk, no disease. It’s that intermediate, those right in the middle that we’re guessing based on their cardiovascular risk, but we’re guessing. So, the coronary calcium score is such a nice way of being able to know right away what their risk is. And for those that are not aware of what a coronary calcium score is, it’s essentially just a CAT scan that detects and quantifies that calcification within the coronary artery. And it’s a marker for the presence or extent of that coronary atherosclerotic plaque.
And I love how – remember the South Beach diet? Arthur Agatston is the one who did the diet, but he also created the scoring. And the scoring just enables to give the provider and the patient or client, the number, the quantity of the calcifications, that is within the artery. And so, you certainly can have a zero, which shows no calcifications at all, or a high number, which shows a significant amount of plaque burden.
But that helps us identify that person who’s at risk. And even better, the individual who maybe might’ve been hesitant about lipid-lowering therapy, or even more so wasn’t ready to quit smoking and lifestyle changes.
All of a sudden, now that they can see the calcifications, the plaque that’s within their arteries, all of sudden now they are much more motivated, ready for a lifestyle change, for utilizing all these different products that can help prevent a catastrophe, a cardiovascular event.
Binu Koirala (Guest): Thank you, Kim. And just to add some more onto that, I think the best approach for the management of higher LDL-C depends on various factors.
For example, individual context such as lipid labels, health conditions, other risk factors, and risk scores that Kim mentioned, medications, and lifestyle. So, it’s really important for health care providers to understand these factors that affect our patients. And here I really want to highlight one resource the listeners can find that in the show notes, which highlights that effective assessment and management of LDL-C is important.
And for that, we really need to work closely with our patient. We really need to work closely with our patient to identify the risk, identify the patients who are at the highest risk of ASCVD.
Also to recognize the need for lipid lowering therapies, which is either statin or non-statin therapies. And then overcoming the barriers we discussed, such as like access, concern over side effects. So, all those things would be discussed and talked with the patients together to identify the intensity of the therapies that is needed to reach the goal of lowering the LDL-C levels for these patients.
And so, the treatment of high cholesterol is really lifelong process. And once an effective treatment plan is set up, it is really important to get committed to that and those plans and reevaluation and follow-up. So hence, I really want to highlight here that involving patients since the beginning and continuing these discussions and treatment plans and revaluation process with them will be really helpful in the LDL-C management.
Geralyn Warfield (host): I really appreciate that both of you have spoken about almost the individualization of the treatment and the discussions and we’re going to talk a little bit more about that.
But before we do, I would like us to really consider as you are meeting with patients, their family members, their caregivers, sometimes they come armed with a lot of information. They have spent a lot of time online. They have done some, I’m going to use air quotes here, “research,” sometimes from areas or were from sources that are not exactly accurate.
So how can we help our patients by helping them understand what misinformation is out there? How can we combat that misinformation, particularly when it comes to this really important topic of LDL-C? Kim, would you like to get us started?
Dr. Kimberly Prado (Guest): Absolutely. Well, for starters, I could say this podcast is perfect for combating that misinformation because it has the evidence-based guidelines, research studies to back it, terrific resources. The PCNA offers so many incredible resources on their website.
At least that is for like the healthcare component.
But you are 100% right. I’ve had so many individuals come in with especially the dietary confusion that’s out there is so prevalent. And individuals want to know what type of dietary recommendations do they need to lower their risk.
And based on the recommendations that I’ve seen is Mediterranean diet is still strong; certainly, consuming a plant-based Mediterranean diet helps with lowering that LDL. And avoiding that damaging, inflammatory trans fats. Want to avoid those trans fats, hydrogenated oils, sugars, sweeteners, refined grains, processed red meats – the processed ones. That is key because they’re so inflammatory. And so, kind of teaching your clients about diet is key because that plays a major role in helping them get to their LDL targets.
So, plant-based healthy fat oils like avocado oil, olive oil, all of those are terrific as an anti-inflammatory benefit.
Also, the DASH diet for those with high blood pressure also gives a nice benefit effect with lowering sodium, increasing potassium.
And there are so many great software applications out there that make it so much easier for patients now. Just off the top of my head, like MyNetDiary. Instead of, in the old days, we used to have to write down all our foods for like the dietician or the providers, the nurses, and write them down, all the salt and everything. Now, all these apps, all you have to do is use your phone and scan the product and it immediately incorporates all the nutrients, the salt content, every aspect of it and calculates it based on what your need is. So, there are some great products out there that clients can use to make their life so much better.
And even with physical activity, many of them are coming in very unclear what to do. And we know that exercise is so beneficial in helping getting that LDL to goal, because of its improvement in insulin sensitivity, enhances detoxification, reduces stress, reduces chronic disease. So, it’s the cornerstone of cardiovascular health.
So, you’re absolutely right. There’s a lot of misinformation, but hopefully between the different apps out there, the podcasts like you’re doing today, hopefully we can help combat that misinformation.
Binu Koirala (Guest): And another approach I’m thinking is shared decision-making. So, our patients come to us. And we work with our patient and their family members. So, we can use some of the tools for shared decision-making to decrease that misinformation or those thoughts they have, or they learned from somewhere.
So, the goal of shared decision-making is to reach into the shared decision or the treatment plan which works best on the available evidence as well as the recognizing the needs and values and experience of the individuals. So, it can also help improve or promote the equity in care and to achieve the treatment adherence as well as improve the health outcomes among our patients.
So, studies have found that shared decision-making is helpful and is a valuable tool for improving these kinds of outcomes in patients. But the challenge is adoption of shared decision-making into routine practice remains inconsistent. As well as there is less guidance on the practical application—we don’t know how to do it, or we might be doing it, but we are not sure we are doing it or not.
So, there is more information we need on these tools and practical application methods on shared decision-making, which might really help us working with the patient and their family members to identify the goals for LDL management. And with this podcast, I have shared a paper which talks about some SDM models and approaches that was recently published from American Heart Association as scientific statement.
I just want to highlight one approach they mentioned there. It’s called SHARE approach, S -H -A -R -E, where S means secure patient participation, H is help patient explore and compare treatment options, A means assess patient’s values and preferences, R, reach a decision with patient, and E means evaluate your patient’s decision.
So, if we exercise these things with our patient, it helps them feel valued, them feel heard, as well as we understand their need, their background, their sociocultural background, maybe diet pattern, because diet has more influence, as Kim said. So, we can understand all those factors and set up a plan that works best for the patient to reach decreasing goal of LDL-C levels. So, I think shared design-making is really one important approach.
Geralyn Warfield (host): I have one final question for each of you, and that is, what would be your top takeaway for our listeners about today’s topic of lowering LDL-C? Kim, why don’t you go ahead and get us started?
Dr. Kimberly Prado (Guest): Absolutely. So, my key takeaway would be atherosclerotic cardiovascular disease still remains, unfortunately, the leading cause of morbidity and mortality, but we have the ability to prevent and preventative strategies by promoting a healthy lifestyle, optimizing a healthy anti-inflammatory diet, promoting physical activity, stress reduction, especially in this crazy world that we’re in sometimes, with meditation apps like MindSpa (great application), and avoiding secondary smoke.
So, lifestyle plays a powerful role and also, very importantly, early detection. The early intervention with that coronary calcium score as a diagnostic testing, lipid and serum biomarkers like that Lp(a), ApoB, or LDL particle, all makes a huge difference. And with that coronary calcium score doing it before any symptoms arise as a preventative test, that is key.
And, certainly, by doing this, that early detection should enable those clients to receive the preventative treatment for early stages of coronary disease that might otherwise have gone untreated and potentially cumulated into a cardiovascular event. So, we have the ability to prevent. everything we can do to do it early is the way to go instead of reacting.
Binu Koirala (Guest): And my last message is, as Kim said, we need to identify the patient at risk of ASCVD, higher risk of ASCVD, and then we need to optimize the dose of available lipid-lowering therapies in combination with the statin. And importantly, we need to practice person -centered approach by utilizing shared decision-making that might help achieve LDL-C target and address this global burden of ASCVD.
Geralyn Warfield (host): As Binu described earlier, we do have information that’s available to you in the show notes, so make sure you check that out for additional resources and more pertinent information that we couldn’t get to in our limited time today.
I am so grateful and would very much like to thank our guests, Binu Koirala and Kim Prado, for sharing their perspectives with us and sharing great resources that we can use in the clinic, hopefully this afternoon or maybe tomorrow morning, depending upon when you’re listening.
I’d also like to thank Amgen for their support of this particular episode.
This is Geralyn Warfield, your host, and we will see you next time.
Topics
- Atherosclerotic Cardiovascular Disease (ASCVD)
- Lipid Management
Published on
September 17, 2024
Listen on:

PhD, MGS, RN

DNP, AGPCNP-BC
Related Resources
Online Interactive Guides
Cholesterol: Journey to a Healthier Lifestyle Online Interactive Patient Guide
February 12, 2025