The updated March 2026 Guideline on the Management of Dyslipidemiai provides a clear framework for healthcare professionals and their patients to effectively address cholesterol management, which has long been a focus of reducing risk for cardiovascular disease.
The updated cholesterol guideline includes clarification on prevention and treatment strategies, goals, and strategies to ensure the best outcomes for patients of all ages.
Eight key takeaways include:
- Earlier management of dyslipidemia, with an individualized approach across the lifespan
- Use of the PREVENT-ASCVD equations to guide decision-making
- Treatment goals for LDL-C and non-HDL-C
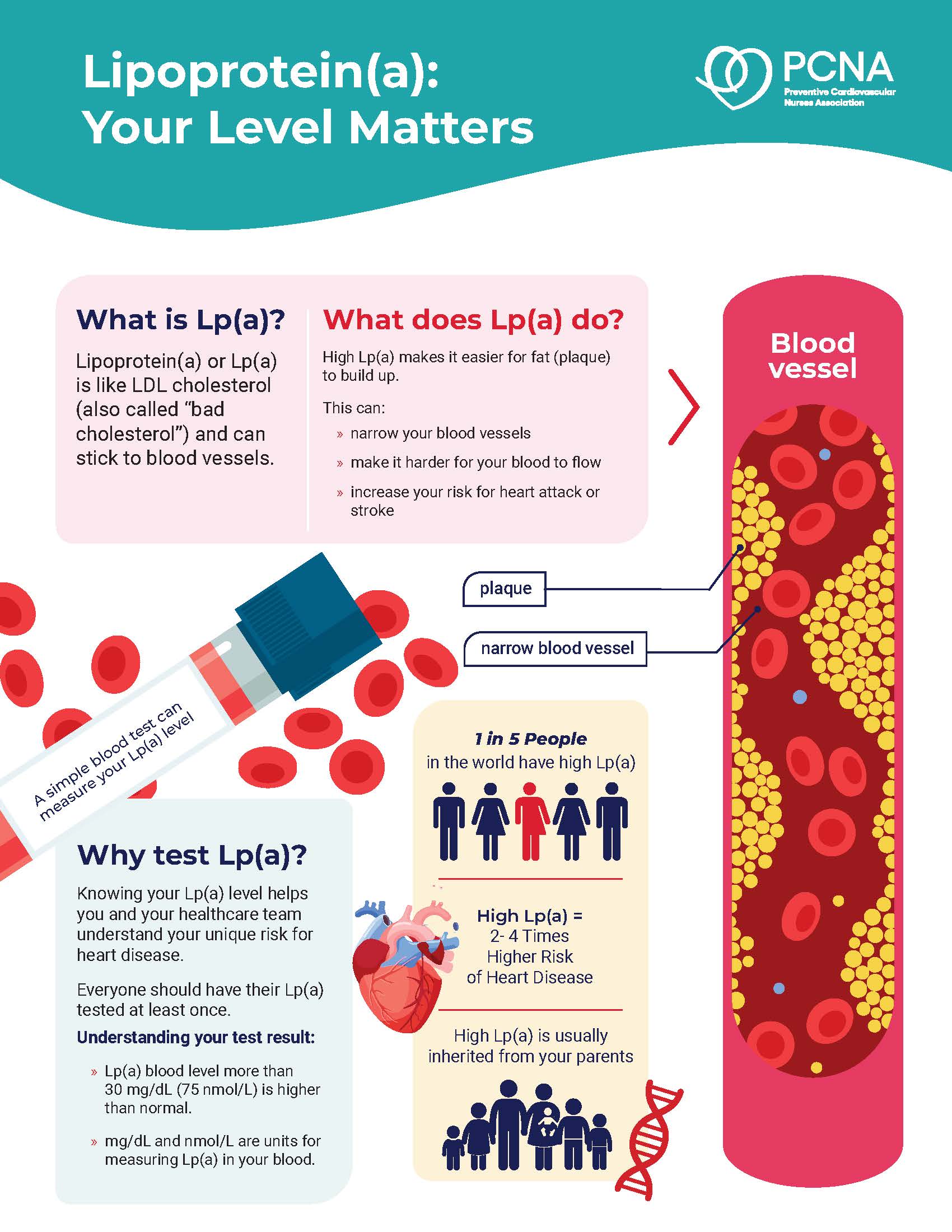
- Lp(a) measurement—at least once
- Selective use of coronary artery calcium (CAC) scoring to refine risk
- Updated recommendations for testing ApoB
- Hypertriglyceridemia treatment
- Combination therapy for lipid-lowering for those not meeting goals
Learn more about the specifics, and how to apply them in clinical practice, below.
1. Dyslipidemia Management Starts Early in Life
Cardiovascular disease is highly preventable, and prolonged exposure to atherogenic lipoproteins can increase overall risk of dyslipidemia and related morbidity and mortality. Healthy habits starting early in life can have positive life-long implications, and it is important to note that it is never too late to start following recommendations for heart-healthy eating, activity, tobacco cessation, adequate sleep, and control of hypertension and other related risk factors.
Supporting healthy lifestyle habits for all patients should start when they are young. For youth with familial hypercholesterolemia (FH), and young adults with LDL-C ≥160 mg/dL or strong family history of premature ASCVD, additional consideration should be given to pharmacotherapy to avoid long-term risk.
Healthcare professionals should use an individualized approach with their patients, regardless of age. Utilization of shared decision-making techniques, and patient-centered care, engage patients in their care and may lead to improved outcomes.
2. PREVENT-ASCVD Equations
As a first step in ASCVD risk assessment, the PREVENT™ (Predicting Risk of cardiovascular disease EVENTs) calculator should be used instead of the older Pooled Cohort Equations (PCE) for those ages 30-79 without known ASCD or subclinical atherosclerosis, and with LDL-C of 70-189 mg/dL.
The PREVENT equation may be used to calculate 10-year risk in those ages 30-79, and 30-year risk in those aged 30-59.
Use the Calculate-Personalize-Reclassify (CPR) model to identify and explain risk.
- Calculate: Use the PREVENT equation
- Personalize with other considering factors such as:
- Risk enhancers (family history of premature ASCVD, chronic inflammatory diseases, persistently elevated triglycerides, elevated Lp(a) or hsCRP)
- Reproductive history (preeclampsia, premature menopause)
- Long-term LDL exposure.
- Reclassify when treatment decisions are uncertain, especially in those with borderline or intermediate risk (3 to <10%) to identify appropriate treatment recommendations
- Coronary artery calcium (CAC) data (more detail in section 5 below)
- CT scans
- CCTA in select high-risk groups (e.g., HIV, T1D or T2D, inflammatory disorders)
3. Lipid-lowering Therapies
Treatment goals have returned to help guide lipid-lowering. In addition to identifying the 10- and/or 30-year risk with the PREVENT™ equations, the updated guideline recommends new thresholds for the initiation of lipid-lowering therapies.
After a clinician-patient conversation, lipid-lowering therapies for LDL-C in adults (modified from AHA Top Take-Home Messages) as recommended below.
| Risk Category | PREVENT 10-year risk estimate | Lipid-lowering therapy | Statin intensity | LDL GOAL (MG/DL) |
|---|---|---|---|---|
| LOW | <3% | Lifestyle emphasis; statin is reasonable for LDL-C 160-189 OR 30-year risk ≥10% | Moderate | < 130 |
| BORDERLINE | 3 to <5% | Consider statin after clinician-patient discussion, assessment of risk enhancers | Moderate | ≥30 to 49%; LDL-C <100 and non-HDL-C <130 |
| INTERMEDIATE | 5 to <10 | Initiate statin | Moderate (at least); for higher end of this risk range, high intensity is beneficial | ≥30 to 49%, with ≥50% beneficial at high end of range; LDL-C <100 and non-HDL-C <130 |
| HIGH | ≥10% | Initiate statin | High | ≥50%; LDL-C <70 and non-HDL-C <100 |
4. Looking at Lp(a)
Lp(a), which is not part of a typical lipid panel, should be measured at least once, as at ≥125 nmol/L (50 mg/dL) it is associated with a 1.4x increased risk. At levels ≥250 nmol/dL (100 mg/dL), the risk is 2-fold higher.
For those with elevated Lp(a), a more intensified LDL-C lowering treatment is indicated, along with management of other risk factors.
5. Considering Coronary Calcium Scoring
In men ages 40+ and women ages 45+, coronary calcium scoring can improve risk assessment and guide treatment goals. The results help to reclassify the risk in adults, both the absolute amount of CAD, and the corresponding standardized percentile, which is currently based on age, sex, and race.
6. All About Apo(B)
Testing of ApoB can also help assess risk and help guide therapy once LDL-C and non-HDL-C goals are met. This is particularly true for those with triglycerides >200 mg/DL, diabetes, or low-achieved LDL-C of <70 mg/dL.
Using only the standard lipid profile may miss residual risk from elevated lipoproteins. Assessing ApoB may also be useful in diagnosing specific lipid and lipoprotein disorders.
7. Handling Hypertriglyceridemia
To reduce ASCVD risk for those with persistently elevated triglycerides, statins remain the foundational treatment in addition to lifestyle.
Treatment for the prevention of pancreatitis may also include therapies to lower triglycerides, particularly in patients with levels ≥1,000 mg/dL (11.3 nmol/L).
8. Considering Combo Therapies
Intensification of lipid-lowering therapiesshould be guided by ASCVD risk and degree of LDL-C lowering achieved. If LDL-C goals are not achieved in adults who are high risk on maximally-tolerated statin therapy, adding ezetimibe and, when appropriate, a PCSK9 inhibitor or bempedoic acid is reasonable.
Considerations for Cardiovascular Nurses
- Secondary prevention of ASCVD will have long-term positive impacts on our patients. We simply need to partner with them throughout the lifespan to support these efforts.
- Thanks to newer therapies that can lower even residual risk, individuals of all ages have a stronger chance of living longer, healthy lives.
- Along with encouraging healthy lifestyle habits, addressing risk at earlier ages, and treating hypercholesterolemia sooner rather than later, can reduce overall risk for ASCVD and lead to lower rates of morbidity and mortality from this highly-preventable condition.

PhD, MHS, RN, FAAN, FAHA, FPCNA

PhD, MPH, RN, CDCES, FAHA, FPCNA, FAAN
Related Resources
Online Interactive Guides
Cholesterol: Journey to a Healthier Lifestyle Online Interactive Patient Guide
February 12, 2025