")
Ruth-Alma Turkson-Ocran PhD, MPH, RN, FNP-BC, CNE and Maria Bonanni CRNP discuss renal denervation treatments for resistant hypertension, including case studies.
This episode is supported by Medtronic.
Episode Resources
Welcome to Heart to Heart Nurses, brought to you by the Preventive Cardiovascular Nurses Association. PCNA’s mission is to promote nurses as leaders in cardiovascular disease prevention and management.
Geralyn Warfield (host): Welcome to today’s episode where we will take a deeper dive into treatment approaches for resistant hypertension. If you would like more background information about hypertension, including resistant hypertension, we encourage you to listen to our previous episode.
Today, I am so grateful to have Maria Bonanni and Dr. Ruth-Alma Turkson-Ocran joining us, and I’m hoping Maria, you could start us off by introducing yourself.
Maria Bonanni (guest): Sure. My name’s Maria Bonanni and I’m a Nurse Practitioner at the hospital of the University of Pennsylvania, which is an AHA-certified hypertension center. My practice primarily focuses on managing patients with resistant and difficult to control hypertension within our Renal [00:01:00] Hypertension Department here.
Penn has worked actively in renal denervation trials for over a decade. I joined the team around 2019, so I’ve been working in renal denervation trials for about the last five years. And personally served as a sub investigator, for multiple RDN trials. I’m absolutely thrilled to participate in this podcast, particularly as we dive into renal denervation, which is an intervention that can really transform the landscape of hypertension management.
Geralyn Warfield (host): Thank you ever so much. Dr. Turkson-Ocran, could you please introduce yourself to our audience?
Ruth-Alma Turkson-Ocran (guest): I am Ruth-Alma Turkson-Ocran. I’m a Clinical Investigator and Instructor of Medicine at Beth Israel Deaconess Medical Center and Harvard Medical School. I’m also a board-certified Nurse Practitioner, and I’m one of the nurse practitioners in our American Heart Association-certified Hypertension Clinic.
I also do a lot of research in this area, [00:02:00] particularly around hypertension prevention, management, social determinants of health, and also in the health equity space. It’s such a pleasure to be on here talking about renal denervation today.
Geralyn Warfield (host): Well, let’s begin talking about hypertension, in particular resistant hypertension, and the role of renal denervation in that particular diagnosis. Maria, could you start us off with that overview?
Maria Bonanni (guest): So, I think to start, you know, it’s important to know that hypertension is a global health crisis. It affects about a third of the global population and half of the population in the US, equating to about 1 billion people worldwide. And despite its prevalence, blood pressure control rates remain low with only about a fourth, or 25%, of all patients who have high blood pressure having controlled blood pressures.
And, alarmingly, there’s studies that have been published that these rates of control are actually decreasing.
Current treatment recommendations for patients who have hypertension [00:03:00] are medications and lifestyle modifications. And we know that medication adherence is a major issue. And in some studies, non-adherence rates are up to 30 to 40% in patients who have hypertension.
So, given that our current approaches to hypertension are falling short, there’s a pressing need for innovative strategies like renal denervation to improve patient outcomes.
So, the concept of renal denervation dates back to the early 1920s and 30s when researchers observed the relationship between the renal nerves and blood pressure. At that time, surgical approaches such as sympathectomy, which involved actually removing the sympathetic nerves, was initially attempted to control hypertension. But these procedures, as you would expect, were invasive and associated with significant risk.
So, following these same principles, catheter-based renal denervation was invented at the beginning of the 21st [00:04:00] century. Catheter-based renal denervation targets the same nerves around the renal arteries.
And we’ve learned a lot more about the physiology of hypertension. So, we know activation of the renal sympathetic nerves causes a host of pro-hypertensive effects, including renin secretion, increased water and sodium re-uptake, and vasoconstriction. And these factors all increase blood volume, thus blood pressure, and drive further renal injury by promoting greater renal afferent firing to the nervous central nervous system.
And renal denervation, through the ablation of the renal nerves, aims to sever the connection between this essentially overactive sympathetic nervous system and the kidneys, thereby reducing blood pressure. Given that this ablation targets both afferent and efferent nerve fibers, renal denervation may also disrupt the afferent firing, thereby lowing global sympathetic activity.
I think that’s a long answer to your question, [00:05:00] but I think, given the reason to consider renal degeneration is the high rates of hypertension, particularly uncontrolled hypertension, in patients. And then this would be really another tool in our arsenal as providers to help reduce blood pressure and therefore reduce the risks of hypertension like strokes, heart attacks, kidney failure, heart failure.
Geralyn Warfield (host): What does the actual process of renal denervation look like?
Maria Bonanni (guest): Sure. So, the patients get referred to, at least at Penn, our cardiology office, and we set them up to meet with one of our interventional cardiologists to plan for the procedure.
The procedure takes place in the cath lab, so as I mentioned earlier, it’s a procedure where they access the femoral artery in the groin, and then they thread a catheter up to the kidney arteries. During this time, the patient is awake and given conscious sedation, so patients are breathing on their own; anesthesia is not involved. And then, depending on which catheter is used, the procedure is slightly different, but essentially the [00:06:00] denervation occurs.
There is some pain with the procedure itself, so patients, are given pretty hefty doses of pain medication. I don’t work in the cath lab, but that’s what I’m told. And patients afterwards don’t complain of that, don’t remember the pain. But, just as an FYI, there is some pain when that energy is, given to the kidney arteries for the denervation.
The patients are usually kept, you know, after the procedure for a few hours. You know, again, the artery access will make sure that it’s not bleeding, that it’s healed, and then the patients, most often go home the same day. I have heard that some patients, you know, during the procedure when you’re given the medication, immediately post the procedure, blood pressures are much better, but most often that’s because they’re given, you know, sedative medications.
So, I think patients come out and they think, “Oh, great, my blood pressure’s 110/70.” But it, you have to think about all the medications that they were given to kind of relax them. and again, so we think that the efficacy or the response in blood pressure does take several months after the initial [00:07:00] procedure.
That’s generally what the procedure looks like in most places.
Ruth-Alma Turkson-Ocran (guest): So, yes, renal denervation is actually a really promising approach for treating resistant hypertension. We had spoken about resistant hypertension in the previous episode or previous podcast. And resistant hypertension is essentially when someone is on at least three different medications, including, a diuretic, just very briefly, but their blood pressures are still not at the target.
So, whether the target, based on their medical history is, you know, less than 120/80 or less than 130/80, you’re still not getting to that target. And so, we can consider renal denervation as a treatment that is complementary for the most part, or in some people, very few people, it can be an alternative to even medication.
And these are [00:08:00] a smaller subgroup. With these people, they may be persons who have medication intolerances, or maybe just the pill burden that they have just to get to, you know, control is maybe very overwhelming to them. And so, these are, so again, can be complementary to anti-hypertensive medications in the quest for achieving, blood pressure control among persons who have resistant or refractory hypertension.
And renal denervation, there have been several—and I’ll talk about it in detail, a little more detail, in a little bit—but there have been several renal denervation, single arm proof-of-concept studies that have shown that blood pressure significantly decreases with renal denervation.
There have been some other studies that have also used, sham control trials, that’s using the more second generation or the newer [00:09:00] renal denervation devices—for example, the radio frequency or ultrasound-based devices—and these have also really shown really good evidence for lowering blood pressure with and without the use of concomitant anti-hypertensive medication.
And I’m sure Maria will talk about the safety profile, which is really good, too.
Geralyn Warfield (host): We’re going to take a quick break and we will be right back to discuss some specifics about the devices.
Geralyn Warfield (host): We are back with our continued conversation about renal denervation as a treatment for resistant hypertension. Maria, could you please share a little bit more about the types of devices that are currently available?
Maria Bonanni (guest): Sure. there are two, recently FDA-approved technologies in catheter-based renal denervation.
One is a catheter that uses radiofrequency ablation. It’s Medtronic’s Simplicity Spyral™ System.
And the other is an [00:10:00] ultrasound-based denervation through Recor’s Paradise® Ultrasound system.
Both technologies achieve the same goal, which is reducing sympathetic nerve activity, in the renal arteries. As Ruth Alma has, you know, previously mentioned, the FDA approval is quite broad and so it’s actually going to be interesting to see how to see how patients are chosen to receive renal denervation.
The FDA indication, really the language, just states it’s used to reduce blood pressure as an adjunctive treatment in patients with hypertension for whom lifestyle modification and anti-hypertensive and medications do not adequately control blood pressure.
So, you know, in a lot of these earlier trials we excluded certain patients. And so, I think this, you know, really broad indication will allow a lot of patients to get treated potentially.
So, I think one of the things that we need to talk about is which patients are the right patients. And [00:11:00] so, again, Ruth Alma listed some of those. So, I think clearly those who have uncontrolled hypertension despite, you know, guideline-driven therapies, patients who have medication intolerances—I ‘m sure you see lots of these patients where they have a list of 15 medicines that they can’t take, and that really limits pharmacotherapy—or those patients, you know, and you even mentioned this, patients that maybe just don’t want to take medications or are very, you know, their pill burden is unacceptable for them. So, I think it does include a lot of different subsets of patients,
Geralyn Warfield (host): Dr. Turkson-Ocran, could you tell us just a little bit more, you alluded to earlier some of the studies that have been done about renal denervation. Could you expand on that just a little bit more and broaden our perspective in terms of how we studied this and how we got to these types of patients as potential individuals who might benefit from this?
Ruth-Alma Turkson-Ocran (guest): Right. So, I would say that the studies for renal [00:12:00] denervation, or I guess renal denervation, is not exactly new. There’s been studies spanning at the very least a couple of decades, for that.
And so, there are, we can talk about maybe the first generation, devices that were radio frequency devices. Essentially, it’s a unipolar electrode on a flexible, you know, catheter, think about maybe like a four French catheter.
And, in the SYMPLICITY trial, hypertension, the first trial that was in 2009, they used this device. And this essentially established that, or determined that, renal denervation was feasible. And in persons who had, whose blood pressures were above target, you could actually see a drop in about 27 points—when I say points, it’s [00:13:00] millimeters of mercury—and so, for the systolic blood pressure. And then about 17 points again for the diastolic blood pressure. That was in the intervention group control compared to the control group.
And this drop in blood pressure or the decrease in blood pressure was still evident after about a year after the procedure.
And so of course, in the research world, we always want to kind of see that, okay, did this really work? And so, there were some people or some criteria that the SYMPLICITY-1 trial did not exactly cover, and so they did a SYMPLICITY-2 trial. And they also saw that blood pressure also decreased significantly again in here, about 32 points for systolic blood pressure in people who had treatment-resistant essential hypertension here.
And so, [00:14:00] to again, in order to address some of the, you know, shortcomings, or the limitations in the SYMPLICITY HTN-2 trial, they went ahead and did a SYMPLICITY HTN-3 trial.
And this was much larger. It was a multicenter, single blind, randomized sham controls trial. However, this trial would, didn’t really, end up meeting its endpoint because, they didn’t necessarily see a statistically significant drop in blood pressure with renal denervation.
However, this also birthed another study, which was called the DENERHTN or the Diagnostic Evaluation of Renal Denervation for Treatment of Resistant Hypertension—that’s a mouthful! And this was, so this trial was a prospective randomized, controlled trial and, [00:15:00] actually gave us really encouraging results for renal denervation
And so, again, in this trial, participants were randomized into, you know, the renal denervation, I guess, intervention, which really was a catheter-based approach. And they also had the control group who essentially continued to receive their regular medication. It was called the standardized step care, anti-hypertensive treatment group.
And so, received their, so patients who had resistant hypertension also received the renal denervation alongside, you know, the standardized stepped care, anti-hypertensive treatment. And so, persons in this particular group, I guess we saw a really significant decrease in systolic blood pressure after six months [00:16:00] because the, that was the outcome, “What was your systolic blood pressure after six months?”
So, we saw about a 13-point decrease, in this particular group compared to the group that was only receiving the standardized step care, anti-hypertensive treatment. And so, these results, again, were just really encouraging and essentially showed that renal denervation used alongside, you know, medication, may essentially offer additional benefit for lowering blood pressure among persons who have resistant hypertension.
Maria Bonanni (guest): Thanks, Ruth Alma, I think that’s a great summary of kind of the data thus far, I just wanted to kind of pick out a few things to kind of focus on.
So, I think when I’m trying to think about counseling my patients on whether or not they should, you know, consider renal denervation, clearly, we haven’t talked about, but you mentioned in your previous episode about secondary causes. So, we really would want to make sure that [00:17:00] we’ve evaluated everyone for secondary causes of hypertension, as well as rule out things like non-adherence, for example, or white coat hypertension. So, we always like to make sure that we’re, you know, screening for these things.
But what I try to counsel my patients when I’m talking about renal denervation is that we do think that most patients respond. So, when we look at all the trials across, you know, we think about 70% of patients respond. So, I do try to tell patients, that, you know, we think most likely that you’ll respond. We can’t guarantee it.
I had a patient that came to me yesterday actually, that told me, “My doctor told me I could be on half of the meds I am on today if I go for renal denervation. So, I have to go as soon as possible.” So, I think expect setting expectations is super important.
And then, like you mentioned, so you know, when we think about the trials that have been published, we think that six months mark, you know, where most of the trial’s endpoints are, we see about a 5-7 mm Hg drop on [00:18:00] average for patients.
And then there are some longer studies that showed duration of treatment and efficacy up to about three years. And we can even see more of a response in blood pressure. So, a drop of, on average, around 18 mm Hg over time. So really exciting. But again, I think it’s really important that patients understand that it doesn’t necessarily mean we’re going to cure your hypertension. We’re not going to necessarily reduce meds, right?
So, if patients are coming in with blood pressures of 150 on four meds and now we can reduce it by say, 20 mm Hg, it’s still, now you’re at goal, right? So, I think that’s really important because I think there’s a lot of information and misinformation out there.
Ruth-Alma Turkson-Ocran (guest): Exactly.
Maria Bonanni (guest): And so, I think as providers we need to make sure that we’re providing that information to our patients, and you know, making this shared decision with them.
Ruth-Alma Turkson-Ocran (guest): Right, exactly. And I absolutely love the fact that you’re talking about, you know, expectations. And I think sometimes people focus on [00:19:00] the medications that people take, but I think, maybe in this case, maybe some redirection, to be looking at, okay, what are your, what are the figures?
And so, you may have to, you may end up being on, you know, your full dose, but then be at target with renal denervation. You know, you may end up having to reduce your dose, but again, be at target or you mean end up not, you know, getting off your medications. And in our clinic, you know, we’ve seen, you know, that range and you’re talking about, you know, 70% of people actually get to have their blood pressures being at target.
And so, with the other 30% who don’t end up being at target, and having to maybe decrease or alter their medications, our goal is okay, you need to be, your blood pressures need to be a target because of the long-term cardiovascular impact [00:20:00] that it does afford.
So, yeah.
Maria Bonanni (guest): Yeah, totally agree. And I’ll just make the last point that, you know, I think sometimes when you tell patients 5-7 mm Hg, they kind of scoff at you, right? They’re like, “Oh, this isn’t a big deal.” But you know, it is important. As you mentioned for the cardiovascular risk.
Ruth-Alma Turkson-Ocran (guest): Right, exactly.
Maria Bonanni (guest): So, we know that there’s like population-based studies that show even a 5 mm Hg drop in blood pressure can reduce cardiovascular outcomes by about 10%. And similarly, a 10 mm Hg drop about a 20% reduce in all-cause mortality. So, I think even though these numbers seem small, they obviously have, they can have a huge impact.
Ruth-Alma Turkson-Ocran (guest): Exactly. I love that you mentioned that.
Geralyn Warfield (host): So, we know that not every patient that comes to you might be a great candidate for renal denervation. How do you determine who is going to be a good candidate? What kind of qualities are you looking for? And also, are there any safety concerns related to this treatment?
Maria Bonanni (guest): Sure, I can jump in. I kind of mentioned some of the patients that kind of come to mind. [00:21:00] Again, since the FDA indication is quite broad, the kind of four groups of patients that I think about, again:
- Uncontrolled despite, you know, guideline-based therapies
- A pill burden that’s unacceptable for patients
- Those with medication intolerances
- One I didn’t mention before is those with increased cardiovascular risk, you know, maybe prioritizing them.
And then, when we think about safety, renal denervation procedures are generally considered safe, with very low rates of complications, particularly when they’re performed by experienced interventionalists in appropriate patients.
Geralyn Warfield (host): My next question for you is what kind of workup is needed for prepping a patient for renal denervation?
Maria Bonanni (guest): So, yeah, the things that we think about, as you mentioned earlier, and that was, you know, more just thoroughly discussed in the previous [00:23:00] episode, is to rule out secondary hypertension. So, things like hyperaldosteronism, renal artery stenosis, fibromuscular dysplasia, pseudo resistance, non-adherence, white coat hypertension or white coat effect, obstructive sleep apnea.
So, I always like to rule out hyperaldosteronism with a renin, actually renin activity level as well as an aldosterone level. Both drawn through the labs to rule out primary hyperaldosteronism, which is a secondary cause of hypertension.
And send them for some type of renal imaging to look for renal artery stenosis, whether that be a renal doppler, if they’re kind of normal or low risk, or if they’re at high risk for renal artery stenosis, maybe send them for a CTA or MRA to rule out renal artery stenosis.
Get a sleep study potentially, and then I always like to confirm their out of office control, whether that be through the use of a 24-hour ambulatory blood pressure monitor [00:24:00] or some home readings. That’s kind of my first, you know, step as far as evaluating patients for RDN.
Geralyn Warfield (host): So how does this look in clinical practice? Could you walk us through a couple of examples?
Maria Bonanni (guest): Sure. So, there’s a few patients that I’ve treated recently that I think would be kind of good general examples.
So, there’s a patient that I follow who’s 52, so young. He has a history of hypertension since his late teens, and hyperlipidemia, as well as a history of CHF many years ago, with a now recent normal, echocardiogram.
He has a strong family history of CAD and I’ve been following him for many years. He’s on 5 antihypertensive meds, including Olmesartan, hydrochlorothiazide, eplerenone, a clonidine patch, and a beta blocker, all at maximally tolerated doses. He doesn’t tolerate calcium channel blockers. and so his pressures at home have always just been a smidge outside of where we’d like them to be. So maybe in the 140s/90s area,
[00:25:00] He works in construction, so he’s very active, and moves around a lot. And he’s very adherent with his medications. But, you know, as a young man, father and busy worker, he has always wanted to have 1) better controlled pressures to goal as well as 2) less medications.
So, we referred him. He was treated about three months ago. And I actually just saw him in clinic and his blood pressures at home have been in the more of the 120s/80s. And actually, sent him for a 24-hour ambulatory cuff, where his blood pressures were actually more in the 120s/70s.
So, I think that, you know, he’s doing really well. His blood pressures are coming down and we’re still early on in treatment. So, I think the goal would be potentially reducing the number of his medications. But I think regardless of that, his blood pressures are definitely now, at goal and at target. And being a 50-year-old man with family history of heart disease and other things, I think, ultimately this is going to reduce [00:26:00] his risk and, set him up for better outcomes in the future.
The other patient that’s a little less straightforward, that always gives me anxiety and palpitations, is this young woman that I follow, she’s 48. And when I first met her, she was actually on 8 antihypertensive medications, most at max doses, with blood pressures in the 180s, 200s. And so, you know, has history of LVH, she’s had retinal hemorrhages.
She actually had some evidence of some mild primary hyperaldosteronism. And given that we did send her for renal, excuse me, for adrenal vein sampling, which didn’t lateralize and so couldn’t offer her any treatment there. But really have struggled for many years with this patient who has, you know, clear end organ damage from her anti, excuse me, uncontrolled hypertension.
And is very adherent. I’ve actually called her pharmacy many times to confirm adherence. Has lost weight, has done all of the things. But again, blood pressure is [00:27:00] severely uncontrolled.
She’s not one of the patients that would’ve qualified for the earlier clinical trials given her evidence of primary hyperaldosteronism, but because we really didn’t have anything else to offer this young woman, we sent her for renal denervation, and she’s been doing fantastic.
So, her blood pressures have been in the 140s/80s, which again, isn’t goal, but for her is excellent and goal for me, and definitely a big win.
So, I think that’s a patient, again, I think, you know, the one thing that I didn’t mention earlier is that we don’t know which patients are the 70% of patients, right? So, we’ve done lots of subgroup analyses of the patients that have been treated in trials, and we’re not sure—is it someone’s race, ethnicity, other groups, excuse me, other diagnoses, gender? We don’t know any of these. You know, we’ve looked into these subgroups and haven’t found the perfect patient.
The one thing that we have seen in the clinical trials is that patients that start with higher [00:28:00] blood pressures, if they respond, they respond more significantly, or the blood pressure drops can be greater in those types of patients.
So, I know the patient example isn’t really like the standard patient, but it’s a patient that I’ve been thinking about many times over the last few years of knowing her. And so, it’s been really rewarding to be able to offer her this opportunity.
Ruth-Alma Turkson-Ocran (guest): This is absolutely, you know, wonderful. I guess we, not with as many specifics as you have, but just to kind of add to what you, have also said, we again…I can just think about two patients that we did have.
Both were male. One was in his early 50s. The other was in his, mid-60s.
Both of them underwent renal denervation.
The younger [00:29:00] one actually ended up coming off all their medications, with blood pressures at targets, so less, you know, in the 120s/80s range.
However, the other one did not end up coming off their medication. I mean, it’s still, we’re still within the six months. I do believe, six months’ time, but we haven’t yet seen any kind of decrease. Their blood pressures have decreased, yes, but they’re still under their preprocedural levels of blood pressure medication.
And so, this just kind of goes back to our previous point about, you know, you have 70, you know, the 70 versus 30% of people who, may end up still—you know the 30% still end up being on their medications, but they may still, even, still see drops in their blood pressures, but they may have to just end up staying on medication.
But, you know, we are still in the [00:30:00] process. And so just kind of looking forward to seeing what things may change. And, on one hand, you know, is the question is it just because maybe the person was older, had just been in that state for, you know, a much longer time and so, you know, it was reversibility an issue?
I feel like we need more studies in that area, to be able to kind of get a better profile, like Maria was saying about, I guess people who maybe this might be beneficial for, versus, versus not. But regardless, these are just really, really encouraging.
Geralyn Warfield (host): We often talk about the importance of team-based care and how does that apply in working with these particular patients?
Ruth-Alma Turkson-Ocran (guest): So, I guess I would start, and then I’ll just let Mary continue. But, when, I guess healthcare in general should not be done in isolation. We do have [00:31:00] experts in, you know, in different areas here. I know our group personally, we do have, in our Hypertension Clinic, we do have, you know, pharmacists who we work with who also help with titrating, you know, blood pressure medications. And, again, nurse practitioners, as well as physicians in our group.
And, I love 1) working with a pharmacist because yeah, absolutely a wealth of knowledge in terms of, you know, medication dosage, whether, you know, whether does this dose transfer to that dose but also, 2) just the insight from whether the physicians or the nurse practitioners, pharmacists, for example, in managing someone, getting them closer to target and then if not, you know, still, working them up, making sure that they’re properly worked up to rule out secondary hypertension, and then work [00:32:00] up for renal denervation.
But. Maria, I’ll let you just go more into details with that.
Maria Bonanni (guest): Yeah, no, I totally agree. Unfortunately, in our program we don’t have access to a pharmacist and I’m very jealous of those who do because they’re amazing from what I hear. and I do work with them in some other aspects of what I do, but I don’t have them, at my fingertips in our hypertension clinic.
But no, I totally agree. I think, you know, team-based care is really crucial for these patients, and I think particularly as centers adopt renal denervation. So, you know, I’ve done a lot of work talking about setting up a hypertension program and about the AHA’s hypertension kind of certification and how that can be really helpful and how can make your program strong, and even be more marketable for patients that are around you geographically.
But I think regardless of if you have the ability to, you know, actually apply and achieve the AHA Certification center, it’s important to set up some type of hypertension [00:33:00] center at your, place of…at your hospital system, because it’s important that you identify the key players. Who’s going to be seeing these patients, managing these patients?
So, you know, a procedure is a procedure. But I think we need to figure out who’s going to be seeing these patients before, making sure that they’re good candidates, making sure that that secondary workup has been done, that the expectations have been set., you know, do the procedure and then who’s going to be following them?
So, I think these are all really important things that need to be ironed out, as I’m sure a lot of health systems, and providers, and interventionalists want to, you know, adopt this new therapy for patients. So, I think team-based care is super important, and I think it’s particularly important as we’re adopting a new technology.
Geralyn Warfield (host): I have one more question for each of you, and that is, if you had one quick takeaway from today’s conversation, what would it be? Dr. Turkson Ocran, how about you?
Ruth-Alma Turkson-Ocran (guest): Great. So, I would say [00:34:00] that, there are options in the hypertension treatment, I guess realm, outside of lifestyle and medications that we can also look to in order to improve blood pressure control rates.
And renal denervation is one of the options—either, you know, we had talked about very rarely alone, but most often, with medication. We can work together with persons whose blood pressure trends may be considered under the resistant, in the resistant, I guess, category. And then looking look into seeing whether or not renal denervation is an option.
We have seen people completely not need blood pressure medications as a result of renal denervation, but we’ve also seen blood pressures get to target levels, or levels considered control, with both medication and renal denervation. Again, everyone is different, [00:35:00] and people need to talk to their primary care clinician for what plan would be best for them based on their history.
And what we have seen so far with the research, and also anecdotally and in clinic, is that the results that we have seen, or been seeing, with renal innovation has certainly been encouraging.
Geralyn Warfield (host): Maria, how about you?
Maria Bonanni (guest): Sure. So, renal denervation, you know, presents a really exciting approach in hypertension management and has the potential to revolutionize how we address one of the world’s most prevalent diseases.
So, it’s proven efficacy, safety, and durability are promising. However, it’s crucial to recognize that the reduction in blood pressure may be modest and not all patients will respond equally. Thus, it’s imperative for patients to maintain, excuse me, to maintain realistic expectations and for providers to engage in shared decision making.
Additionally, ongoing [00:36:00] patient follow up is necessary to better understand which individuals benefit most from this intervention.
Geralyn Warfield (host): We are so grateful to you both, Maria Bonanni and Dr. Turkson-Ocran, for being with us today and sharing a little bit more about this process of renal denervation, which patients might be those that benefit most from this particular type of treatment. And so, thank you so much for sharing your expertise with us.
We’d also like to thank Medtronic for their support for this episode.
You can find links to the resources and also to the trials that we discussed in this episode in the show notes.
This is your host, Geralyn Warfield, and we will see you next time.
Thank you for listening to Heart to Heart Nurses. We invite you to visit pcna.net for clinical resources, continuing education, and much more.
Topics
- Atherosclerotic Cardiovascular Disease (ASCVD)
- Hypertension
Published on
April 16, 2024
Listen on:

CRNP

PhD, MPH, RN, FNP-BC, CNE
Related Resources
Online Interactive Guides
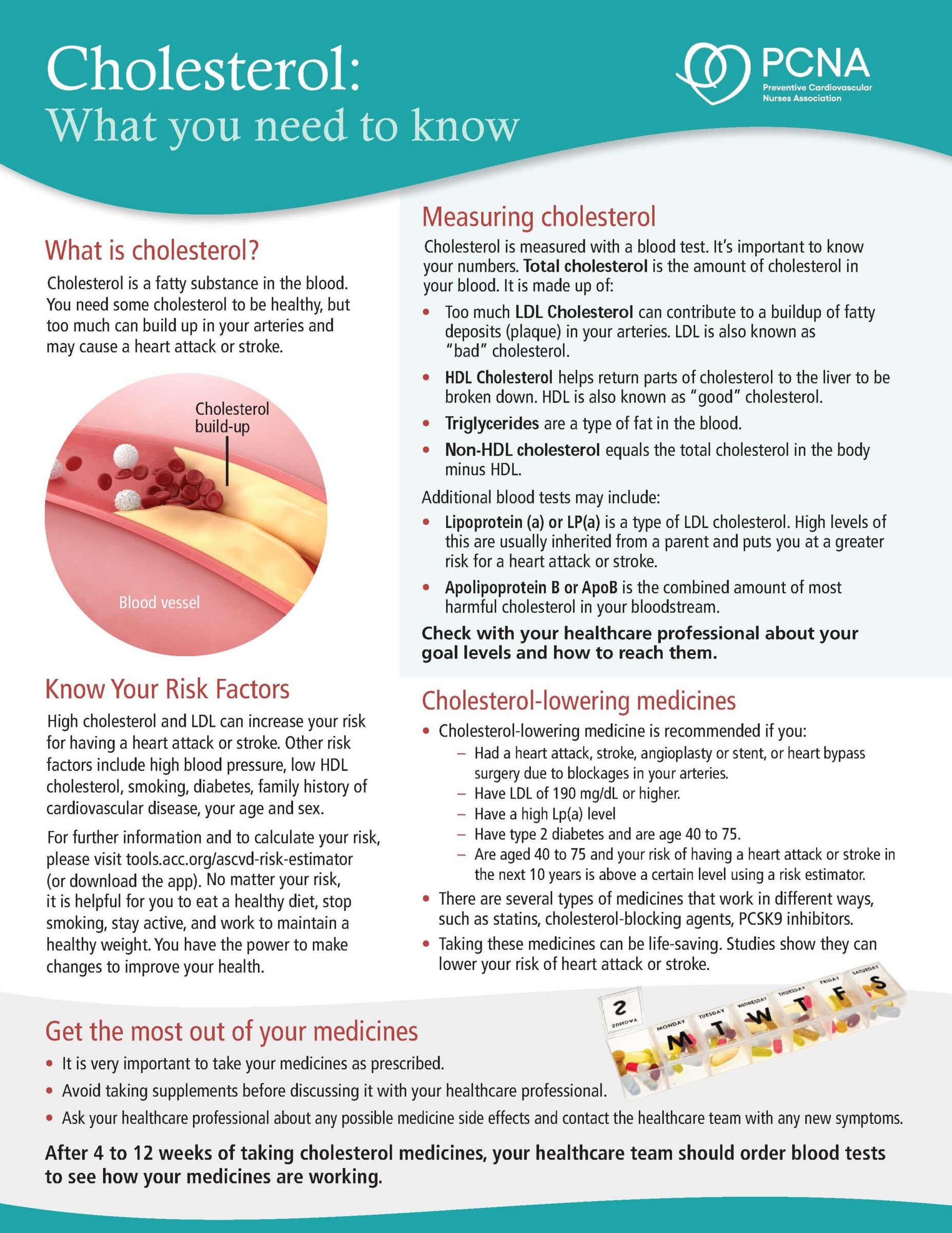
Cholesterol: Journey to a Healthier Lifestyle Online Interactive Patient Guide
February 12, 2025