Guests Mary Janette Sendin, MSN, APRN-CNS, CCNS, PCCN, and Daniel Weinstein discuss the patient journey for those with PSVT and the challenges that can delay diagnosis for some individuals. The importance of patient-centered care in the healthcare setting and beyond is also part of the conversation.
Take 1 minute to tell us what you think about this episode.
This podcast episode was supported by grant funding from Milestone Pharmaceuticals.
Welcome to Heart to Heart Nurses, brought to you by the Preventive Cardiovascular Nurses Association. PCNA’s mission is to promote nurses as leaders in cardiovascular disease prevention and management.
Geralyn Warfield (host): Welcome to the second of a three-episode miniseries focused on paroxysmal supraventricular tachycardia, also known as PSVT.
In our previous episode, we discussed episodic rapid heart rate conditions. And in the next episode, you’ll be able to hear about treatments. But in this particular episode, we’re going to focus on the patient experience and the importance of patient-centered care.
In today’s episode, we’ll also be talking a little bit more about the patient journey. And we are really grateful to have a patient with us, and that is Daniel Weinstein. And we also have a healthcare professional with us, Janette Sendin. Jeanette, could you please start us off by introducing yourself? [00:01:00]
Janette Sendin (guest): Yes. Hi. Hello everyone. My name is Janette, and I am an Advanced Practice Registered Nurse and a Clinical Nurse Specialist role with cardiology.
And I work a lot with electrophysiology patients. And I have been in this role since 2012. And I have been in cardiology since, I believe, about 30 years. And it is a privilege to be part of this special part of the podcast.
Geralyn Warfield (host): Thank you so much, Janette. Daniel, could you please introduce yourself to our audience?
Daniel Weinstein (guest): Good morning. I’m Daniel, and I’m super excited to be here with you chatting about PSVT. I am, for my day job, I am a chef and, despite my PSVT, I’m still pretty active. I’m a mountain biker, a scuba diver, and I’m sitting in my garage right now because I’m halfway through the [00:02:00] process of converting my garage to a pottery studio.
Geralyn Warfield (host): Wow, Daniel, that’s an exceptional array of activities that you keep yourself busy with, even with PSVT.
So today, as I described earlier, we’re going to talk a little bit more about the patient journey and patient -entered care.
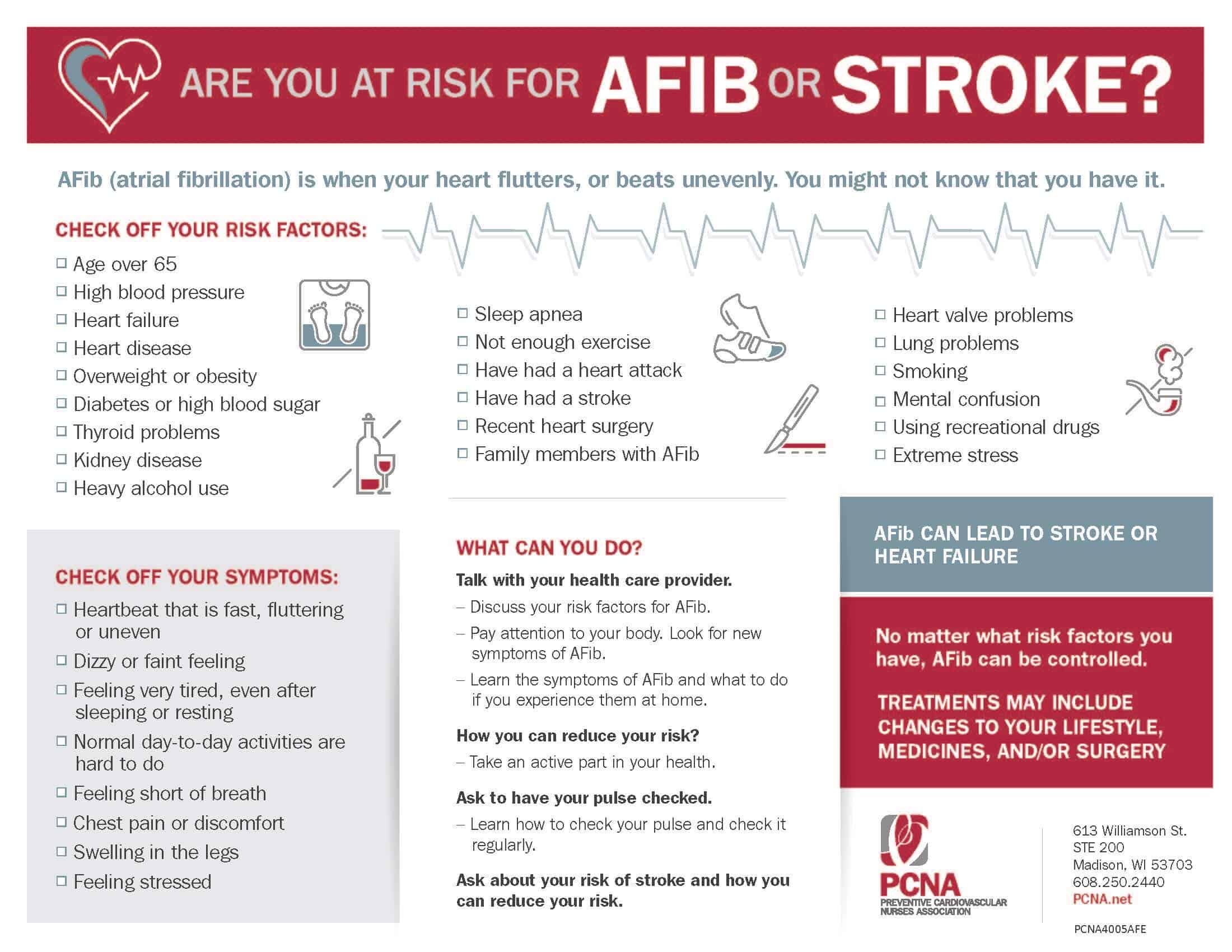
And for those of you that are a little less familiar, I just wanted to give a brief review of what PSVT is. Simply put, it’s when an individual’s heart rate intermittently beats regularly, but very rapidly, and that’s due to an issue somewhere in the upper part of the heart. So, Daniel, can you tell us what your experience has been with PSVT?
Daniel Weinstein (guest): Yeah, I had my first episode when I was 16, so that was quite some time ago. I’m 53 now, so I’ve been living with it for a long time.
That first episode, you know, took me by complete surprise. I was running around, just goofing around in the hallway with my friends, Jenny and Elvin. Just running and [00:03:00] laughing and, you know, having a good old time and suddenly look, bam, you know, I describe it as, your whole body feels this big kind of jolt.
It’s a soft jolt. It’s not, it’s like being hit by a freight train covered in cotton balls.
Your heart rate, my heart rate, goes from, you know, around 75 and instantly, not gradually, but instantly goes to about 180, just from one beat to the next. So, you certainly feel it through your whole body.
That first time I was, I was absolutely, you know, terrified. And I, I just sat down on the floor and my friends were kind to me and they said, “Are you okay?”
And I said, “I don’t know.” That’s pretty much all I could say at that time. I don’t know what’s going on.
Janette Sendin (guest): So, Daniel, I bet that was a very uncomfortable experience that you’ve had.
Just tell me, what tests were [00:04:00] performed to confirm your diagnosis? At that time, did you see an electrophysiologist, who are the specialists of the electrical side of the heart?
Daniel Weinstein (guest): Yeah, the, the first specialist I saw was a cardiologist and he, said, “OK, it sounds like you’ve got this thing, called PSVT.” and he put me on a heart monitor, I guess an EKG.
And despite that, he still couldn’t be sure if I had PSVT because, apparently, it turns out that you can’t actually tell that someone has this condition unless they happen to be experiencing an episode while they’re on the EKG.
So, he said, “Yeah, you probably have this thing called PSVT and, good news, it’s not too dangerous. It’s not fatal. It may get worse as you get older.” And then he said, “You know, if you want to, we could put you on a [00:05:00] heart monitor to, you know, a portable heart monitor, to see if we can actually capture an episode, but if not, you know, nothing much we can do. Good luck, kid. Bye bye.”
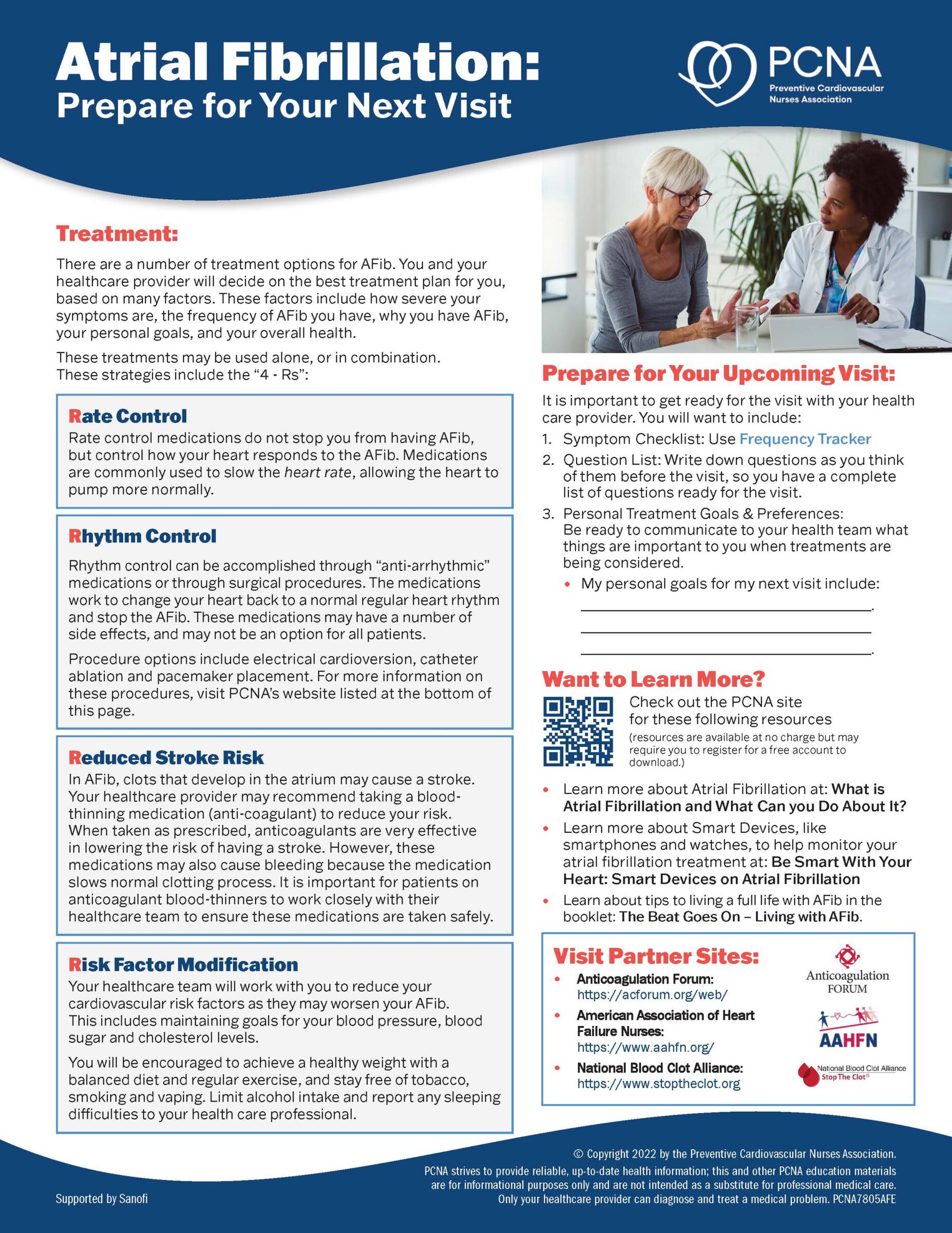
Janette Sendin (guest): OK. So, did they do some sort of an EP ablation, electrophysiology study, like an EP study at that time?
Daniel Weinstein (guest): I don’t know what that is, so I’m going to guess that I didn’t have one. I do know a little bit about the idea of ablations, But you know. I guess in ablation, they sort of destroy one of those nerves that connect to your heart and that can help people with the condition.
Is that, do I have that right?
Janette Sendin (guest): Yes. So basically, so what I was trying to say is, an EP study is basically trying to stimulate your heart and elicit the symptom that you were [00:06:00] experiencing. And then that’s where they’re going to find out where the short circuit is coming from. So basically, as we all know, our heart has our own electrical conduction, like any kind of electricity.
And when you have the circling or short circuit, that’s when they will elicit it during that time of the EP study. And if needs to burn that side that’s causing the circuit, you know, that’s causing your heart to beat fast. that’s when they do the ablation. But it looks like, you know, it looks like you have not had that, am I correct?
Daniel Weinstein (guest): Yeah, that’s right. I have not had that study, nor have I had an ablation. I feel like at this time, you know, my symptoms, my experience with PSVT, I would describe as a pretty mild, pretty lucky case.
I feel like the potential risks of an ablation, although they’re [00:07:00] low, don’t merit the procedure in my case. Because, you know, being a mountain biker and a scuba diver, I’m still pretty active. The PSVT, although I have them (episodes) very frequently, they don’t last very long and I don’t have a lot of complications with them.
So, at this time, I’m not ready to consider an ablation. Maybe as I get older, that’ll be a nice option to be able to consider if my conditions worsen or change.
Janette Sendin (guest): Yes. The greatest part is you’re in a great position. It’s because there’s a lot of innovation, advances in technology and in medicine now that PSVT is not something that is hard to handle.
But I know that every patient experience is different when they are experiencing SVT, a PSVT. What types of symptoms do you currently have when this occurs?
Daniel Weinstein (guest): When I get a PSVT episode, there’s, [00:08:00] there’s no warning at all, except for one heartbeat in front of the PSVT. So, you never know. It’s, it’s absolutely random. Doesn’t seem to have anything to do with my sleep, or my diet, or my coffee, or my stress. It’s absolutely random.
And then when it does come on, I feel sort of, I might describe it almost as a skipped heartbeat. I don’t think that’s what’s really happening, but that’s sort of what it feels like. And then again, suddenly my heartbeat goes up by about 100 beats per minute. and then usually that’s just about it. Just that heart beating rapidly.
Other folks can, when they have an episode, other sufferers, they can have dizziness and, and shortness of breath and lightheadedness for the most part, I’ve never had that. recently though [00:09:00] I did. Recently I did. I had two episodes in which I got pretty, pretty dizzy.
I’m guessing it’s because I lost quite a bit of weight. I lost 55 pounds. And I had two of those lightheaded episodes. Now, having said that, I’ve had, you know, 25 episodes since those dizzy episodes, and I haven’t had any dizziness. So I, so I don’t know exactly what’s going on, but for the most part, I get the just the heartbeat.
And, I have some techniques that I can try to use. There are sort of standard procedures that PSVT patients are taught: bearing down as if they’re using the bathroom, blowing into a straw with your finger on the end of the straw, kind of pressing your breath inside of you. Those don’t work for me. Putting my feet up against a wall, that doesn’t work for me. Splashing my face with really cold water [00:10:00] (that is a technique that some folks use), that doesn’t work for me. All I can do is kind of sit quietly and just breathe deeply and relax.
But having said that, there are plenty of times when I don’t have that option. if I’m driving a car, If I’m working as a chef at my day job and I have 100 people waiting for some delicious tri tip. If I’m mountain biking, and you know, a couple of times when I was scuba diving, I actually had an episode. So, try to relax and that’s, and then usually it gets better—just when I say usually, it always does. It always gets better.
And in my case, for whatever reason, my episodes generally are pretty short. They can last from 10 seconds to a minute, five minutes. Not much longer usually.
Janette Sendin (guest): Okay. Thank you, Daniel. That was a [00:11:00] very informative sharing that you gave.
I know that a lot of patients rely on technology to track their symptoms. Do you use some sort of a Fitbit or a smart watch to track, you know, how fast your heart rate is going and has this been effective to you?
Daniel Weinstein (guest): I do. I have an Apple Watch and I’m super excited to have an Apple Watch because it’s really cool. It does all kinds of cool stuff. I had a cheaper sort of generic Fitbit type thing, and it actually was unable to keep up with my PSVT heart rate. So, I said, “Oh darn it, I’m going to have to buy a really expensive Apple Watch.” (laughs)
So, I have that, and it does a great job. It can, it can track my heart rate very carefully, whether it’s a regular heart rate or in episodes. And, sometimes, you know, if I’m not wearing it and I have an [00:12:00] episode, I’ll go ahead and put that on real quick and, and then keep an eye on that heart rate.
And it’s really, really cool because for the first time I can watch my heart rate. at the end of an episode, I can see exactly, or pretty closely, what my heart does going from 175 and in one heartbeat down to 75. Again, PSVT, it’s the same on both ends. It doesn’t gradually slow down. It just instantly decreases by 100 beats per minute or so, and it’s cool. It’s pretty cool to see that on the on the watch face there.
And I can record it, also. The software talking to my phone can keep track of that. And then I can show that to my cardiologist.
Janette Sendin (guest): That’s very good. And it’s amazing what technology can do.
Anyway, what additional education have you received, from your provider [00:13:00] about SVT, and also when to seek immediate medical assistance when you feel that you’re eliciting not only the fast heart rate, but other symptoms.
Daniel Weinstein (guest): You know, my doctors, I’ve had, I’ve had a number of cardiologists throughout the years because I’ve had this condition for a long time. And so cardiologists tend to retire and so that I get a new cardiologist and each one brings, you know, new information. That’s really nice because, you know, I get a new perspective from a new doctor.
Cardiologists have, you know, really done a super job of reassuring me that this is not a condition that anyone dies from. I just have to really emphasize that for people who have this condition, that speaking to the doctor, [00:14:00] speaking to people who have experience, it’s so, for me, it’s so helpful and so comforting. I love, you know, to be honest, I love when my cardiologist says for the 50th billionth time, “Don’t worry, Daniel, no one’s ever died from this.” I can’t hear it enough.
So, cardiologists bring information. One of the things that they reassure me, in my case, is I don’t—now this is my case. I can’t speak for any other PSVT patient— in my case, my cardiologist has reassured me that I do not need to go to the emergency room unless I’m experiencing an episode that lasts for something like, you know, 48 hours. That’s again, my case.
Now I have been to the emergency room twice, and I will tell you that no matter what my cardiologist says, if my heartbeat continues to last more than three or four hours, which is [00:15:00] very rare for me. Doctor, my wife takes over. If I have, if I last too many hours, she says, “We’re going to the emergency room.” And so that’s how I’ve ended there twice.
But for the most part, for the most part, you know, having experienced, I don’t know, thousands and thousands and thousands of these episodes, I’ve been at the ER only two times.
Janette Sendin (guest): That’s great. So, you know, as Daniel has described, working with patients, we as healthcare providers, it is essential that we work with our patients and each individual patient is, different, you know, each individual have their own experiences.
We respect their values, their goals, their plans of care. And we work together to come up with a treatment plan that is best for each individual patient.
Geralyn Warfield (host): Thank you so very much, Daniel, for sharing your experience as a patient with [00:16:00] PSVT. We are going to take a quick break and we will be right back.
Geralyn Warfield (host): Welcome back to our discussion about PSVT, where we have a patient, Daniel Weinstein, and a healthcare professional, Janette Sendin, to describe for us a little bit more about patient-centered care. Oftentimes in nursing and other fields, we talk about team-based care and sharing decision making. And we talked a little bit about that before our break, how patients and families sometimes work together.
Daniel, you described how your wife gets involved in your care if she feels like your PSVT episodes are going along longer than she feels comfortable with, even though you might be comfortable with it. And that’s when you trek to the ER. How do you work as a team, I guess I would say, Daniel, with others on the management of your PSVT?
Daniel Weinstein (guest): I’m super lucky. I have so much support. I have my wife, Esther. She has been with me through a good part of this journey. And my wife, I’m sorry, my daughter Taylor, she knows a lot about my condition. [00:17:00]
And I do spend a lot of time, I also play a lot of racquetball and I play with my friend Tracy and she knows about my condition. So, if I’m hitting it hard in the court and suddenly, I have to sit down, she knows how to help me through that.
So, I have a ton of support. And of course, my cardiologist. And I only have to see my cardiologist once a year, but now, you know, it’s again, it’s a really great way to monitor and get reassurance.
Now, the other thing that I’ve started to be able to do, is to make connections with PSVT sufferers from around the country. And just hearing their stories, hearing the way they handle and work and cope with their, with their condition. Each one of those connections just helps me build out my knowledge about PSVT, my understanding of the types of ways a person could experience it. my [00:18:00] understanding of how people, you know, manage when and if they go to the emergency room.
And one thing I’ve noticed chatting with more and more PSVT patients, I’ve noticed this really…I think it’s disturbing: a lot of females say that they had a much harder time getting their condition diagnosed.
I was ,when I was 16 and the doctor said, “It’s probably PSVT.” The story that I’m hearing from females, however, is they’re often told, “That’s anxiety.” “That is nervousness.” “That’s nothing to worry about.” And that, that really concerns me.
So for having spoken to a lot of sufferers, I would just reach out to anybody who is feeling something weird in their, in their chest, in their heart area, make sure to really advocate. Advocate and, you know, [00:19:00] hopefully by getting to know more resources and understand that, you know, this is real, that hopefully they can say to their friends and family and doctors, “There’s something going on here.” “I need some help.” “I need some support.”
Geralyn Warfield (host): So, Jeanette, from your perspective as a healthcare professional, what does patient centered care mean for you? Obviously, Daniel has described the support that he has with his family and with his cardiologist, but how about from your perspective? What does that look like?
Janette Sendin (guest): As Daniel described, working with a patient to ensure that we as healthcare professionals need to listen to the patient’s perspectives. We need to understand and recognize their values, their goals, and we need to work collaboratively to come up with a treatment or management plan that we all pursue for each individual patient. [00:20:00]
We, when healthcare providers work together as a team, like the cardiologists and other specialties, we each can also share our areas of expertise. By working collaboratively with one another, including referrals to specialists, we can ensure that each patient has access to the information and support they need so that we can maximize patient outcomes.
It is important that healthcare professionals stay up to date with the latest guidelines and treatments for SVT. And for any diseases that they care for. Educating patients at risk for their rhythm and making a close loop communication between them and their providers can help further improve the management of the symptoms or these rhythms.
[00:21:00] If available, patient education should always be provided, as well as resources that are familiar to the patients and their families, including online resources and pamphlets. So, in general, treatment of PSVT Can involve an interprofessional team and working collaborative will enhance the outcomes of each individual patient.
Geralyn Warfield (host): Thank you so very much, Janette, for that great perspective from the healthcare. provider or healthcare professional aspect of team-based care.
And I’m wondering if there’s anything else that either of you would like to add that we haven’t previously discussed in this episode. Daniel, is there anything else?
Daniel Weinstein (guest): I want to say that especially for people who experienced their first PSVT [00:22:00] episode, whether they’re young or old, it can be scary. And it’s so nice to know that there are a lot of folks who have a lot of knowledge, and empathy, and resources. I hope that folks experiencing their first episode really feel like they get the support and love that I’ve been lucky enough to have throughout my PSVT journey.
Geralyn Warfield (host): Wonderfully said Daniel. Janette, is there anything else you would like to add?
Janette Sendin (guest): Okay. So as a healthcare professional, one important learning or information that I would like to share is that there’s, with the advances of technology, there’s several treatments out there for SVT. But what is important is each individual, when [00:23:00] experiencing these symptoms, needs to seek expert consultation.
The electrophysiologists are the cardiologists who specializes in this field in taking care of patients with SVT. Hence, it is very important that early diagnosis, early management, and a thorough follow-up of the conditions of patients having SVT, is important.
Geralyn Warfield (host): We are so incredibly grateful to both of you for being here today. Thank you so much, Janette Sendin and Daniel Weinstein, for being part of this three-part episode series on PSVT, and we really appreciate your perspectives on the patient journey and patient centered care.
Don’t forget to listen to the other two episodes in this miniseries. And for more information and resources, please check out the episode show notes and visit [00:24:00] pcna.net for a related video and even more details about PSVT.
Thank you to Milestone Pharmaceuticals for their grant funding for this podcast episode.
And this is your host, Geralyn Warfield, and we will see you next time.
Thank you for listening to Heart to Heart Nurses. We invite you to visit pcna.net for clinical resources, continuing education, and much more.
Topics
- Arrhythmias
Published on
October 3, 2023
Listen on:

MSN, APRN-CNS, CCNS, PCCN, FPCNA
Related Resources