In this second episode of a three-part content series on pulmonary hypertension, we sit down with Raza Farhan, MD, and discuss the journey of diagnosis for PH. Dr. Raza describes the nuances behind pulmonary hypertension WHO groups and dives into right heart catheterization.
Earn 0.3 CE contact hours from listening to the podcast episode and completing the course components.
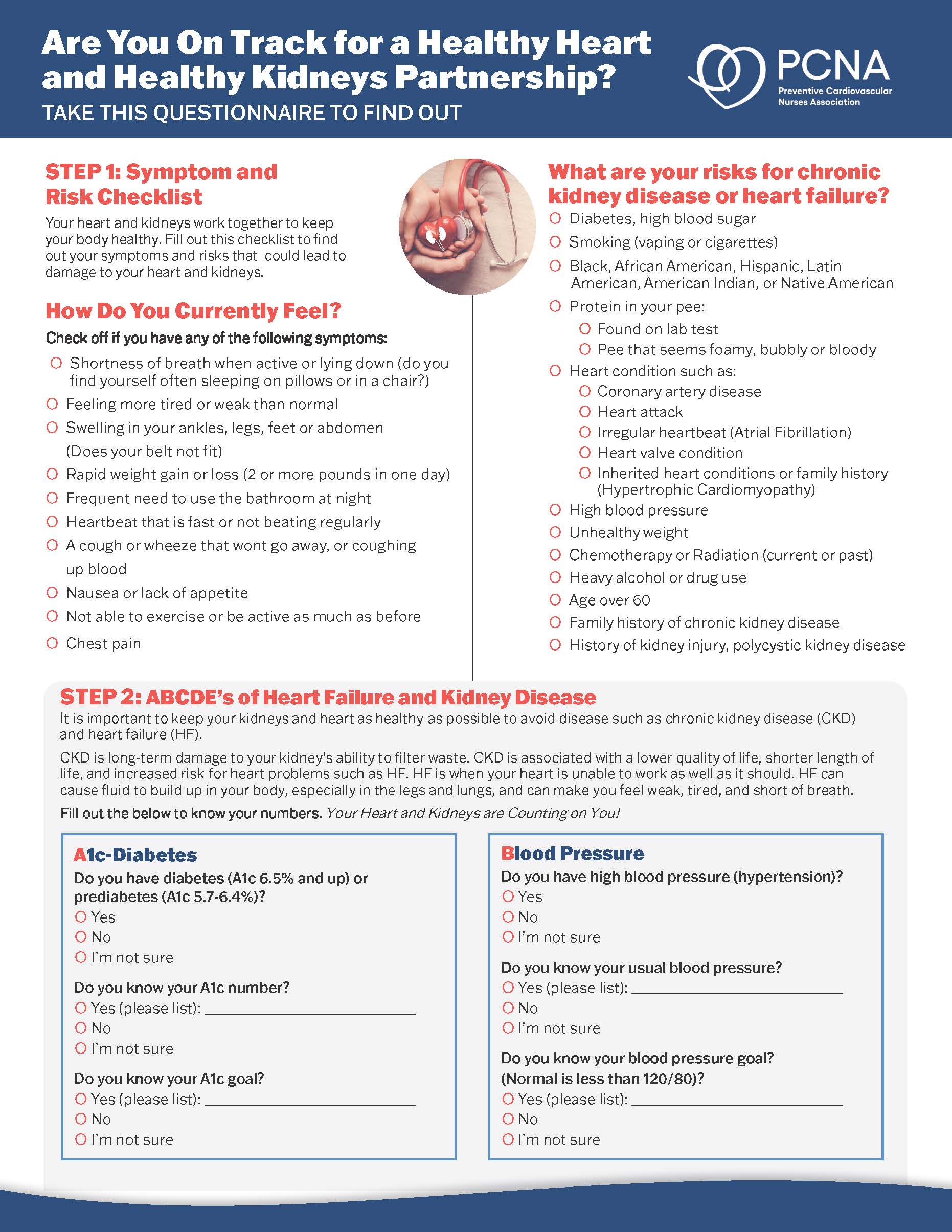
Episode Resources
Welcome to Heart to Heart Nurses. Brought to you by the Preventive Cardiovascular Nurses Association. PCNA’s mission is to promote nurses as leaders in cardiovascular disease prevention and management.
Geralyn Warfield (host): Welcome to today’s episode, the second of a three-episode mini-series on pulmonary hypertension. Our previous episode looked at recognizing pulmonary hypertension and today we’re going to be exploring the next step in the journey of a patient with PH, the diagnosis.
To help us learn more about this topic we’re talking today with Dr. Farhan Raza from the University of Wisconsin – Madison. Dr. Raza, could you please introduce yourself?
Farhan Raza (guest): Thank you for inviting me, Geralyn, I’m delighted to join you today. I’m a pulmonary hypertension and heart failure cardiologist at University of Wisconsin in Madison.
I’ve been practicing PH for nearly 10 years and have been at UW Madison for over four years now. Since arriving here, [00:01:00] I’ve started an exercise physiology invasive cardiopulmonary exercise test lab. We do participate in multicentric clinical trials and have a PH accredited center. We also have quite a few internal research studies in vascular mechanics and myocardial biology here at UW.
Geralyn Warfield (host): I suspect that our audience can tell already that Dr. Raza is an expert at PH and we’re very excited to have him on the program today. I’m hoping that we might be able to start with a global view of things.
Dr. Raza, the World Health Organization or WHO, has described five different groups of pulmonary hypertension. Could you shed for us some light on those five groups?
Farhan Raza (guest): Yes, PH is a very diverse disease. It nearly affects 1% of the global population, hence the need to create this classification. The five groups that WHO created do represent five different types of diseases. So, [00:02:00] we call them W-H-O or WHO groups.
So, WHO group one involves patients who have some type of pulmonary arterial hypertension. It includes idiopathic patients, patients who develop PH due to connective tissue disease like scleroderma. Some of the other common causes are portal hypertension, HIV infections, and drug toxicity.
WHO group two is the most common type that occurs due to some type of left heart disease, and that could be a diverse group of diseases in themselves. In the form of heart failure with reduced rejection fraction or preserved rejection fraction, sometimes related to heart valve disease, like mitral valve or aortic valve disease.
And then WHO group three is related to some type of lung disease that triggers hypoxia. This could be common things like COPD, interstitial lung disease, obstructive [00:03:00] sleep apnea comes under the same category.
And then WHO group four is a very peculiar type of pulmonary hypertension due to thromboembolic disease. More common word that we use is CTEPH. WHO Group four, chronic thromboembolic pulmonary hypertension.
And the last group is WHO Group five. Which is kind of a basket for a lot of different diseases that don’t belong in any other group. So, this could be a multifactorial group of diseases. The more prominent ones that come in this category are kidney failure patients who may be on dialysis and then some other common hematological blood disorders like polycythemia vera come under this group as well.
Geralyn Warfield (host): That is quite an extensive list of diseases that are classified into these five WHO groups! Might there be a more simplified approach to these five groups?
Farhan Raza (guest): Yeah, that’s a great question. I think these groups do give us appreciation for the diversity of PH patients that we deal [00:04:00] with. But thankfully there is a very simplified approach of thinking of pulmonary hypertension as either one of the two bigger problems.
So, the first one, you could call it more pulmonary arterial hypertension. Pathology where the disease is starting in the pulmonary vasculature in the pulmonary arteries or arterials, and that creates high pressure and resistance in the pulmonary circulation. We do call this precapillary pulmonary hypertension as well.
And then the second category are related to some type of heart disease. One could use the words congestive heart failure for those group of diseases or pulmonary venous hypertension or post capillary pulmonary hypertension.
So, most of the WHO group diseases fall in either one of these two categories. Either more of a pulmonary arterial problem with pulmonary arterial hypertension like [00:05:00] disease or a congestive heart failure like disease.
Geralyn Warfield (host): Could you describe for us or elaborate on how you talk to patients who have these two different types of pulmonary hypertension?
Farhan Raza (guest): That’s a very good question also. A lot of times it can be quite challenging for patients to navigate how come they have pulmonary hypertension. They may know somebody else who has pulmonary hypertension, who may be on very different treatments to what treatment suits them.
So, the way I describe to patients is what I briefly described before, that they may have one or the other type of pulmonary hypertension. For example, if I’m dealing with a patient who has pulmonary arterial hypertension, I will describe to them that they truly have damage to their lung blood vessels. They will benefit from different treatments, different drugs that help lower the resistance of pressure in their blood vessel, pulmonary blood vessels, and they may need additional workup for [00:06:00] autoimmune disease or blood clot problems in their lung blood vessels if that is relevant to them.
So, I’ll have that type of conversation with a patient who has pulmonary arterial hypertension.
For the second type of patient who may have essentially congestive heart failure, I will actually use that word to describe to them that that is their primary problem. And that needs care for their heart disease in the form of underlying problems they may be facing [such as] coronary disease, atrial fibrillation, heart failure problems. And I’ll let them know that they do have some type of pulmonary hypertension, but it is a secondary problem, their primary issue is congestive heart failure.
Geralyn Warfield (host): We’ve been discussing pulmonary hypertension and its diagnosis, and we’re going to take a quick break. We will be right back.
Geralyn Warfield (host): We’re back with Dr. Raza to continue our discussion about the diagnosis of a patient with pulmonary hypertension, and I’m hoping we could spend a little bit of time talking about right heart catheterization. What [00:07:00] is that exactly?
Farhan Raza (guest): Very commonly, if we think about the journey that a pulmonary hypertension patient goes through, the patient themselves have been experiencing shortness of breath or inability to exercise for quite a long period of time till they actually seek care through their primary care doctor.
At some point along the way, they get an echocardiogram, which is the ultrasound of the heart that picks up pulmonary hypertension in most of the cases as the, as a screening test. And in some selective cases, the physicians who are involved in the care of the patient, they decide to confirm the diagnosis of pulmonary hypertension through this invasive test.
So that’s essentially what a right heart catheterization is. It is an invasive test. And it allows pulmonary hypertension physicians to simultaneously confirm pressures in pulmonary arteries and estimate [00:08:00] pressures on the left side of the heart. And first of all, confirm that if the diagnosis of pulmonary hypertension is correct, but more importantly, they can identify which type of pulmonary hypertension the patient has.
Geralyn Warfield (host): Could you describe for us how the procedure is done and also what a patient should expect when they come in for that particular test?
Farhan Raza (guest): Yes. So, the procedure is done most commonly in this part of a hospital, which is labeled as heart catheterization or cardiac catheterization lab.
It is pretty standard in most centers, when a patient comes in, they are notified ahead of time just to be fasting overnight. And then they arrive in this part of the hospital where they are welcomed by most commonly a nurse, and make sure they don’t have any kind of acute illness that should or any [00:09:00] concern for bleeding that will create some risk for the procedure.
Once all of that is checked in, the patient is moved to a procedure room and most commonly a cardiologist or heart doctor will start off by placing a catheter or a tube in some specific part of the body. So, we call it an access site for the catheter. Very commonly it can be the site in the groin or in the neck where the jugular vein is.
More recently, we’ve been doing some of these procedures through a vein in the arm as well, we call a brachial vein. So, one of those three options tend to be the most common sites when it comes to access site. The next aspect of this procedure is really the length of the procedure.
So, it roughly takes somewhere between 15 to 30 minutes, but a lot of time is [00:10:00] spent before the procedure in the preparation. Some centers do use some sedative for this test as well, so patients are comfortable and relaxed. But not all centers do that.
And very frequently expert centers like ourselves try to think of some provocative maneuver that is generally done after some of the heart and lung pressures are assessed. So, these provocative manures may vary. So most common one that is done in pulmonary arterial hypertension patients is inhaled vasodilator drugs. So nitric oxide is used in most centers. Prostacyclin is also used in some other centers.
So that is a very common thing done in pulmonary arterial hypertension patients to check if their lung pressures decrease in the short term when this inhaled drug is given in the cath lab.
Some other centers, [00:11:00] including us, do perform exercise testing as well in selective cases when people come in for our right heart catheterization. So that is generally achieved through some type of a stationary bike in either upright position or a supine position. And then the last thing I’ll mention on the topic of provocative maneuver is in, especially in patients who have some type of congestive heart failure, they are given sometimes a slightly different type of drug called nitroprusside. And that attempts to normalize the heart pressures and also the blood pressure to see how the heart and lung pressures may behave.
Geralyn Warfield (host): So, you’ve described three different ways that you might have these provocative maneuvers. Does the length of the test vary based on whether or not you’re using some of these other maneuvers?
Farhan Raza (guest): That’s an excellent question. Yes, so as [00:12:00] I described the actual procedure for the right heart cath may not take more than 15 minutes in most cases. But if you do add on one of these provocative maneuvers that can add another 15 – 20 minutes of the procedure time. For example, inhaled nitrate, which is used very commonly in pulmonary arterial hypertension patients, is based on the protocol by guidelines, the inhaled nitric should run roughly up to 10 minutes.
So, after 10 minutes of the medication used, then you have to repeat the check of these pressures and blood flow, so that adds on at least 15 minutes of procedure time, if not longer.
Geralyn Warfield (host): So, what types of information or results are you seeking?
Farhan Raza (guest): So, the right heart catheterization provides essentially two key pieces of information. One is related to the pressures, and the second piece of information is related to blood flow, we call cardiac output.
And then the [00:13:00] third piece that we actually calculate from these two pieces of information is resistance across the lung blood vessels.
So, if we reference and review the recent guidelines from European Society of Cardiology and European Respiratory Society that were published in 2022, the diagnosis of pulmonary hypertension is based on mean pulmonary arterial pressure.
So, if the mean pulmonary arterial pressure at rest is more than 20 millimeters of mercury, that actually is the gold standard definition of pulmonary hypertension. So that is the first piece of information that we are paying attention to.
The second piece of information is related to an estimate of pressure on the left side of the heart. So, through a heart catheterization, we essentially assess this one specific pressure we call pulmonary artery wedge pressure, and that is a way for us to estimate the pressure on the left side of the heart, specifically [00:14:00] left atrium and essentially within the left ventricle at the end of diastole.
So, the cutoff that is used in the pulmonary hypertension guidelines for pulmonary artery wedge pressure is 15. For example, if your wedge pressure is 15 or lower, that will be normal. But once the wedge pressure is more than 15, for example, 16 or higher, then the patients will have some type of left heart disease. And that’s something we have to take into clinical context.
But that is the second pressure that can really help us guide if we’re dealing with a patient who either has pulmonary arterial hypertension with a wedge pressure equal to or less than 15, or we’re dealing with a patient with congestive heart failure, with a wedge pressure of 16 or higher.
And then the third piece related to resistance specifically we define it as pulmonary vascular resistance. And the cutoff we [00:15:00] previously have been using for pulmonary arterial hypertension has been more than 3. And woods units is the unit that we use, however, in 2022, guidelines by ESC and ERS that cutoff for pulmonary vascular resistance has been dropped from 3 to 2.
So PVR more than 2 would be consistent with precapillary pulmonary hypertension or pulmonary arterial hypertension while, PVR equal to or less than 2 will be consistent with some type of left heart disease or congestive heart failure.
And, I will add on one last comment to that definition; the motivations and the reasoning behind decreasing the PVR cut off from three to two is based on quite a lot of interesting epidemiological studies that really indicated that once the PVR does start to increase [00:16:00] above 2, there is a high risk of mortality among pulmonary hypertension patients.
So, the motivation behind dropping the PVR from 3 to 2 is for early identification of disease in these patients.
Geralyn Warfield (host): Is there anything else that you’d like to add that I neglected to ask already?
Farhan Raza (guest): Those are really I think great, great questions and discussions. I will just add on, um, there are a lot of researchers and societal guidelines out there for pulmonary hypertension.
I do find the 2022 ESC/ERS guidelines for pulmonary hypertension as an excellent resource and it’s open access, It’s available online. ESC and ERS have done a fantastic job of starting off by defining what are the normal pressures and blood flow and resistance in normal people. And when these metrics start to become abnormal, [00:17:00] when one would be labeled with a diagnosis of pulmonary hypertension and they do a fantastic job further defining the type of pulmonary hypertension a patient may have.
And that leads into different treatment pathways as well. So, it can be an excellent guide all in one place.
Geralyn Warfield (host): We would like to thank our guest, Dr. Raza, for our discussion today about the diagnosis of pulmonary hypertension. We’d also like to thank Merck Sharp and Dohme Corporation for their unrestricted grant funding for this episode.
This is your host, Geralyn Warfield, and we will see you next time.
Thank you for listening to Heart to Heart Nurses. We invite you to visit pcna.net for clinical resources, continuing education, and much more.
Topics
- Heart Failure
- Hypertension
Published on
June 20, 2023
Listen on:
MD
Related Resources