Team-based care models are crucial in managing complex disease states such as cardio-kidney metabolic disease. Learn from guests Melissa Magwire, RN, MSN, CDCES, the Program Director of the Cardiometabolic Center Alliance, and Christine Memering, MSN, RN, CDCES, BC-ADM, FADCES, on strategies to overcome barriers and improve patients’ health outcomes.
This episode is supported by Boehringer Ingelheim Pharmaceuticals, Inc.
Episode Resources
Welcome to Heart to Heart Nurses. Brought to you by the Preventive Cardiovascular Nurses Association. PCNA’s mission is to promote nurses as leaders in cardiovascular disease prevention and management.
Geralyn Warfield (host): Welcome to today’s episode where we will be focusing on the importance of team-based care as we’re caring for the complex cardiorenal disease patient. Today I have two exceptional guests with me, Chris Memering and Melissa Magwire. Chris, could you introduce yourself please?
Christine Memering (guest): Sure. I am an inpatient diabetes care and education specialist for the last 17 years. I’ve been an RN for 22 years in the hospital and I’m master’s prepared. I do hold my certification in diabetes care and education, and I hold the board certification in advanced diabetes management so that I can help everyone in my hospital take really good care of people with diabetes and [00:01:00] other chronic diseases. And I am a fellow of the Association of Diabetes Care and Education Specialist.
Geralyn Warfield (host): Thank you so much. Melissa. Could you introduce yourself to our audience please?
Melissa Magwire (guest): Sure. Hi, Melissa Magwire. I am a master’s prepared nurse as well with 35 years in cardiovascular nursing as well as a certified care and education specialist. I practice in a cardiometabolic center of excellence, but then I’m also the program director of the Cardiometabolic Center Alliance.
Geralyn Warfield (host): Well, thank you both so very much for being here today, and we look forward to learning even more about this topic than we did in our first two episodes. Melissa, could you please start us off by ensuring we’re all on the same page when it comes to what that really means in terms of the phrase team-based care in healthcare?
Melissa Magwire (guest): Yeah, I, you know, I think we all agree that when it comes to chronic care and chronic disease management, you really have to have that comprehensive team based essential [00:02:00] background. That’s the only way it’s going to work. Patients are rarely dealing with one disease state, unfortunately. In fact, it’s usually two or three different diseases at the same time.
It’s complicated, it’s confusing, and really being able to navigate that, navigating multiple teams, multiple care plans, really takes a coordinated approach. And there are so many ways that the essential aspects of care teams can be overlooked when, you know, looking at how we model that care, and if we really want the best outcomes, we’ve got to have somebody driving that and really takes that comprehensive approach.
Christine Memering (guest): Yeah, Melissa, that’s right. I mean, my primary focus may be on someone’s diabetes and the care related to that in the hospital, but we all know diabetes doesn’t live in a silo. It affects everything that the blood touches, and any other chronic disease that may be out there in any treatment we may do for that other chronic disease may affect the diabetes and vice versa.
I work in the hospital and you can’t work in a hospital and not work on teams. You know, we have all sorts of different [00:03:00] versions there. So I have a really strong relationship with our cardiology teams, with our nephrology teams, with our different therapies. I did my master’s work in part with the cardiology team. And learned all about how we could, you know, do that team-based approach and shared appointments for people with diabetes and heart failure specifically. But it did help me to create a stronger team with cardiology, with people in the hospital. So now I’m pulled in a little sooner to their care or by the cardiologists themselves and not by the medical team, which is quite helpful.
My favorite team-based care in our hospital is actually our inpatient rehab where we have people working based on the, you know, the patient need, the family need. But we’ve got our therapies, our physical therapy, occupational speech therapy, our clinical social workers, our clinical dieticians, psychology, even down to our TheraPaws team, which is our therapy dogs that come in. And it’s amazing how [00:04:00] that can just release so much stress to somebody who’s been in the hospital for a really long time.
And we work with all sorts of diagnosis within the hospital and have to take into account that whole approach there. And everyone’s got to have the history of everything going on, what the plan is, trying to make those transitions helpful so that we can help people stay healthy and stay out of the hospital. We’re here when you need us, but you know, in the long run, we hope you get to stay home.
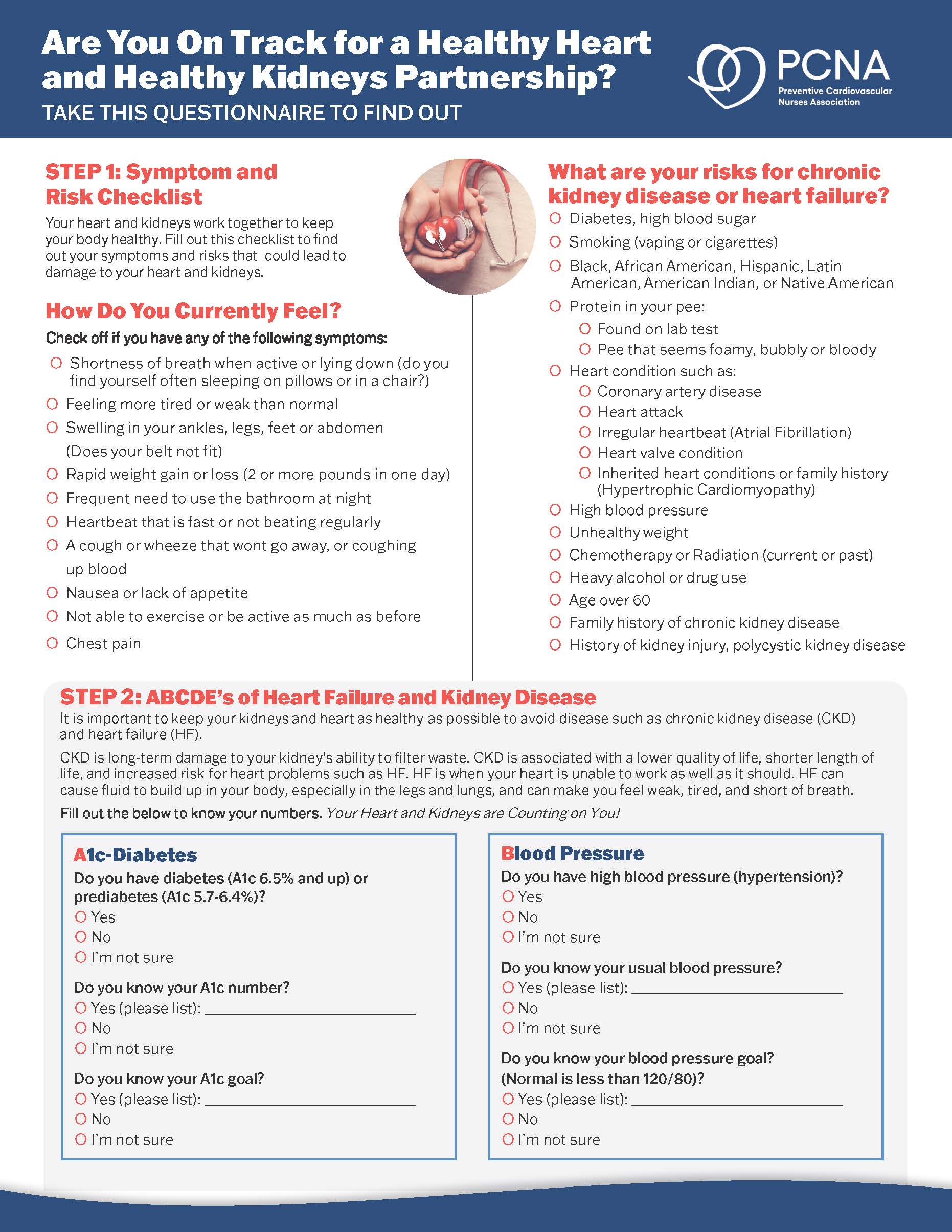
Geralyn Warfield (host): In previous episodes within this mini-series we have discussed the interconnected nature of cardiovascular disease, kidney disease, diabetes, and hypertension.
But one of the components that may not be front of mind for individuals is the role of a healthy liver when it comes to a healthy cardiometabolic system. So I’m not sure who might want to address this for us.
Christine Memering (guest): Well, Melissa, everything I’ve learned about these conditions I learned from you. So I’m going to let you take this one.
Melissa Magwire (guest): Well, I don’t know about that, but we can learn from each other. But, you know, the liver is [00:05:00] so involved in metabolism and we talk about that in diabetes all the time. But really looking at that interconnection of the liver and cardiovascular and looking at liver health as really a cardiovascular risk factor. And some of the ways that’s highlighted recently is we know there’s been a change in the nomenclature recently. From what has traditionally been known as NASH and NAFLD to really needing to recognize the liver as an important consideration in CKM disease management. So now the terms are MASH and MAFLD. With the M standing for metabolically. Metabolically associated conditions, to really tie that in.
So both MASH and MAFLD are associated with increased risk for cardiovascular disease and those living with type two diabetes are at high risk for developing both conditions and more so even related fibrosis. And we know that fibrosis is a strong hallmark of poor cardiovascular outcomes.
One of the things I think is not [00:06:00] recognized is how often this does actually appear. Those living with ASCVD and related comorbidities, um, are really at high risk. And then you take in type two diabetes, which puts folks at about a 20% more increased risk for significant fibrosis. So there really is a need to start recognizing the liver and liver health as a cardiovascular risk component.
Geralyn Warfield (host): So what kind of screening or diagnostic tests do you recommend to assess these body systems?
Melissa Magwire (guest): So both ADA as well as multiple GI societies suggest that anyone living with type two diabetes be screened for fibrosis because of the fact that we just mentioned that those living with type two are at such high risk.
And so a great non-invasive way of doing that is what we call the FIB-4, which is a non-invasive screening tool. And essentially it just takes an AST and ALT and a platelet count. Then gives you a score and you can look those up online. It really gives you a risk equivalent and a score. And if patients [00:07:00] are screened and score as an intermittent or high-risk, additional screening, like a Fibroscan should be considered to actually mark the level of fibrosis that can start as easy as that AST, ALT, platelet popping those numbers into an online version of the test that will calculate the FIB-4. Many EMRs have those embedded as well now.
Geralyn Warfield (host): We are going to take a quick break and we will be right back.
Geralyn Warfield (host): I’d like to welcome our audience back to our discussion, and I think all of us recognize the complexities of healthcare. And whether or not we’re focusing on one body system or more than one body system.
There is a lot to that, but I think one of the things I’d love for us to address a little bit more is the considerations that we need to keep in mind so that our patients don’t fall through the cracks where we are dealing with transitions of care or even transitions of care teams. And Chris, could you address that for us?
Christine Memering (guest): Sure. I mean, in and out of the hospital system creates these [00:08:00] really big areas of transitions of care, whether they’re going back to their home situation or going to a rehab, whether that be subacute or acute for a little while, or just having a completely different home and now being taken care of by somebody else.
So one piece in my practice that I like to include is a chart note to the primary care provider or specialist, especially if we’ve had any big change in the care plan. I was actually at my daughter’s college orientation and had lunch with our local providers and she told me how great grateful she was for notes like this.
The discharge summary can be kind of generic sometime,s is trying to summarize, you know, sometimes a two day stay or a two week stay. And it really may not address the concerns that the patient has had discussions with different members of the care team but wants to follow up with their PCP.
So these little notes of… Hey, I saw your patient, this is what we talked about, here’s where we wanted to go. And oh, [00:09:00] by the way, they’re gonna be in rehab for a little while before they come back to see you… Can really help those transitions and those transitions of care just create these opportunities for thinking about what that patient is expecting in their healthcare with long-term, with different chronic disease pieces going on and you know what that planning may look like. You know, we talk about having a birthing plan for when you’re coming into the hospital to have a baby. And this is the way we kind of want it to go, but honestly, that care planning and personal goals and outcomes of someone managing chronic disease can help to keep those open communication lines during all of those transitions.
Melissa Magwire (guest): I think, I mean, you summarized that beautifully and I think it, like you mentioned before, it really takes a team and it’s that clear communication and you hit that multiple times, Chris, it’s that communication because there are multiple care teams and there are [00:10:00] multiple, you know, comorbidities that these patients are facing. And I recently had a loved one in the hospital and I thought, how does someone navigate this if they don’t have someone who’s used to trying to look for that coordination? And I think that’s where we really need to step in and understand that it’s not just the patient, but it’s the patient support system. But it’s also that peripheral around the patient, their other care teams to understand, okay, this is what we’ve done, this is what the patient’s care plan is, making sure we’re all on the same page. Making sure somebody has that clear view of the goals for that care. And then we know with bringing it back to those CKM conditions, how they’re all interrelated and what your care plan is and what my care plan is, are probably, you know, along the same pathway, the goal and really getting on the same page and understanding that it is all intertwined and inter-related.
Christine Memering (guest): It’s actually something that I hear patients ask for. They feel like nobody’s in that driver’s seat or nobody’s talking to each other and I get this medication added by this person and this medication added by this person. But using the, that patient centered, [00:11:00] person centered care planning can definitely create better open lines of communication and generally leads to better health outcomes as well.
Melissa Magwire (guest): Yeah, and not just for the patient. I think, you know, because you are looking at so many things within that spectrum of their wellness, that other providers understanding why you started certain medications or why you have something in your care plan so that it’s not inadvertently, you know, especially in a transition period, discontinued or not continued, and making sure that you’ve got that full 360 communication.
Geralyn Warfield (host): Those are excellent takeaways that we can actually put to use no matter where we are in our careers, where we are in terms of practice, because our patients do rely on us for some of that navigational skill that we can provide that you are exactly right, Melissa. I’ve had people in the hospital or come to different physicians and get different information, kind of a mixed message, if you will, and having a clear consensus for that is not always possible because there’s so many interconnected parts. So I really [00:12:00] appreciate the fact that this is not an easy linear process, is it?
Melissa Magwire (guest): No.
Christine Memering (guest): Definitely not.
Geralyn Warfield (host): Well, we have talked a lot about a lot of different things thus far, but one of the things I would love for us to spend a little bit of time on is health inequities. We know that they exist, but how does that apply specifically to barriers that might happen in cardio kidney metabolic conditions?
Christine Memering (guest): How much time do we have left in the episode?
I mean, this is a topic that, that can go on and on and should go on and on because I think we’re making a lot of assumptions sometimes. Um, and not always really looking at these health inequities. I think the CDC and others have really tried to help us with this a lot, and it is bringing it much more to the forefront.
I mean, any chronic disease, whether it be a cardio kidney metabolic condition, but housing language literacy, transportation [00:13:00] access, incarceration, income insurance, implicit bias, racism. I mean, if it’s a health inequity, it’s a barrier to cardio kidney metabolic condition, and any other chronic condition honestly.
Melissa Magwire (guest): Yeah, I mean you summarized it fantastically. I mean, it is one of the key hallmarks of care coordination and needs to be right up at the front because you know, it’s all well and good to have a care plan outlined for a patient. But if they don’t have a safe place to exercise, if they don’t have housing, if they don’t have transportation, if they don’t have the funds for “healthy”, you know, meals or the way to do that, they can’t follow that care plan. We need to set that patient up for success, you know, because all want the ultimate goal, which is great outcomes, and if you don’t assess some of these inequities and some of these social drivers of health, then you’re missing one of the key points of your care plan in providing care to these folks.
Christine Memering (guest): We’re actually at our hospital. It is this kind of early [00:14:00] assessment piece, and I think everyone is trying to do it as an early assessment piece because I feel like, and I see this a lot as a diabetes care and education specialist, everyone just kept saying, oh, well, they’re just not following the directions. They’re, you know, we’re not gonna use that word, but, they’re not being compliant with things and really so much of chronic care is looking at the barriers and trying to help understand how they overcome them. And that’s where, what health inequities look at. So if I’ve got someone who is dealing with homelessness and doesn’t have a refrigerator to put their insulin in, you know, how are they going to be expected to manage their chronic disease while they’re trying to do that and get their kids to school, you know? And make sure there, there’s food somewhere?
With all of those pieces, so, I think it helps us to really look at those barriers and remember that these are people and people first. And that is just a huge piece that we should be doing as nurses, especially.
Melissa Magwire (guest): I think [00:15:00] one of the, that’s a lot, and I think one of the sort of statistics that sticks with me is that like 20 to 30% of someone’s health is actual healthcare delivery. How that care is delivered.
But that rest of that 70% to 80% of it’s everything else that you just talked about. It’s all those social drivers of health. So you can have someone in the hospital receiving, you know, the best care ever, but that’s really only 20% of the picture of their health journey.
The rest of it is all of these social drivers of health. So I think to your point, it’s something that needs to be assessed right out of the gate, first and foremost and and really needs to be an integral part of that team communication and that collaborative care model.
Geralyn Warfield (host): I have one final question for each of you, and that would be what’s your top takeaway from our conversation today that you would like listeners to have top of mind for them when we think about the topic of team-based care in Cardiorenal disease?
Melissa Magwire (guest): Yeah. So I think mine is that clear, concise [00:16:00] communication and education is the foundation for everything. And then the other thing, just on a personal note, is every patient needs to be treated like they’re your loved one. And, and what type of a plan and what type of a team would you want your loved one to be on?
Because I think when we put ourselves in that position and understand how complex, you know, having a chronic disease is especially something like chronic, you know, cardiovascular kidney metabolic disease. How you want that care delivered is how you should be delivering it to your patients.
Christine Memering (guest): Yeah. No, I completely agree.
I think I would add advocacy in there a little bit too, because I think we can be not only great advocates for people we’re taking care of at the time, but also just in general with when it comes to policy or how policies within your institution or all those pieces there.
It’s interesting, Melissa, that you [00:17:00] mentioned how much more time it takes to take care of chronic disease. I actually use a Facebook post with all of my new nurses that were training on understanding, really, Type one diabetes. And it was from an 18-year-old who said that every, you know, she woke up at eight o’clock and every time she had a thought about, that was related to diabetes in some way, she made a tick mark on her hand.
And by the end of it, she was up for, and this is an 18-year-old, 15 and a half hours and had 247 thoughts that had nothing to do with being an 18-year-old. They had everything to do with managing their diabetes. And I think it’s really important to remember that, especially when we’ve got all of these chronic diseases coming at like, chronic, conditions coming at us and, and all the different pieces that play into taking care of that.
So that communication, the education, the listening part of communication, and that advocacy, that would be my takeaways.
Geralyn Warfield (host): Well, [00:18:00] if you have not already, we would encourage you to listen to the other episodes in this miniseries for more details about the complexities of cardiorenal health. You can also find more information in the show notes for this episode and at pcna.net.
I am so incredibly grateful to these two individuals for spending time with us today, Melissa Magwire and Chris Memering. Thank you so much for sharing your expertise and your perspectives with our audience today. We’d also like to thank Boehringer Ingelheim Pharmaceuticals Incorporated for their support of this episode.
And with that, this is your host, Geralyn Warfield, and we will see you next time.
Thank you for listening to Heart to Heart Nurses. We invite you to visit pcna.net for clinical resources, continuing education, and much more.
Topics
- Diabetes
- Kidney Disease
Published on
August 20, 2024
Listen on:
RN, MSN, CDCES

MSN, RN, CDCES, BC-ADM, FADCES
Related Resources
Online Interactive Guides
Diabetes and Your Heart: Close Connections Online Interactive Patient Tool
June 12, 2025